

La lordosis y la escoliosis son dos afecciones distintas de la columna vertebral que pueden afectar a personas de todas las edades. Aunque ambas afecciones implican una curvatura anormal de la columna vertebral, difieren en cuanto a sus características únicas, causas, síntomas y opciones de tratamiento. Comprender las diferencias entre lordosis y escoliosis es crucial para un diagnóstico preciso y un tratamiento eficaz de estas afecciones. En este artículo, profundizaremos en los detalles de cada afección, explorando sus causas, factores de riesgo, síntomas, diagnóstico, opciones de tratamiento y posibles complicaciones.
¿Qué es la lordosis?
La lordosis, también conocida como swayback o hiperlordosis, es una afección caracterizada por una curvatura excesiva hacia dentro de la columna vertebral en la zona lumbar. Esta curvatura anormal hace que las nalgas sobresalgan y que el abdomen parezca más prominente. La lordosis puede afectar a personas de todas las edades, pero es más frecuente en niños y adolescentes durante la fase de crecimiento.

Causas y factores de riesgo de la lordosis
Hay varios factores que pueden contribuir al desarrollo de la lordosis. Una de las causas principales es una mala postura, sobre todo cuando se está sentado o de pie durante periodos prolongados con la pelvis inclinada hacia delante. Otras causas potenciales son la obesidad, el embarazo, ciertas afecciones neuromusculares como la distrofia muscular y las anomalías congénitas de la columna vertebral.
Ciertos factores de riesgo pueden aumentar la probabilidad de que una persona desarrolle lordosis. Entre ellos se incluyen un estilo de vida sedentario, un aumento excesivo de peso, determinadas ocupaciones que requieren estar sentado o de pie durante mucho tiempo y ciertas afecciones médicas que afectan al tono y la fuerza musculares.
Síntomas y diagnóstico de la lordosis
El síntoma más notable de la lordosis es una curvatura exagerada de la zona lumbar hacia dentro. Esto puede provocar un abdomen y unas nalgas prominentes. En algunos casos, las personas con lordosis pueden sufrir dolor lumbar, rigidez muscular y dificultad para permanecer de pie mucho tiempo. En casos graves, la lordosis también puede afectar a la marcha y a la movilidad general del individuo.
Para diagnosticar la lordosis, un profesional sanitario suele realizar una exploración física, evaluar el historial médico de la persona y puede solicitar pruebas de imagen como radiografías o resonancias magnéticas. Estas pruebas ayudan a determinar la gravedad de la curvatura y a identificar cualquier causa o complicación subyacente.
Opciones de tratamiento para la lordosis
El tratamiento de la lordosis depende de la gravedad del trastorno y de la presencia de causas subyacentes. En los casos leves, las modificaciones del estilo de vida, como mantener una buena postura, hacer ejercicio regularmente para fortalecer los músculos centrales y controlar el peso, pueden ser suficientes para aliviar los síntomas y evitar una mayor progresión.
En los casos más graves, puede recomendarse fisioterapia para mejorar la fuerza muscular y la flexibilidad. En algunos casos, puede prescribirse un corsé ortopédico para proporcionar apoyo y ayudar a corregir la curvatura. En casos excepcionales en los que la lordosis provoca un dolor importante o problemas de movilidad, puede considerarse la cirugía para corregir la curvatura y estabilizar la columna vertebral.
Complicaciones y efectos a largo plazo de la lordosis
Si no se trata, la lordosis puede provocar diversas complicaciones y efectos a largo plazo. Entre ellos, dolor de espalda crónico, desequilibrios musculares, mayor riesgo de lesiones de la columna y disminución de la movilidad. Además, una lordosis grave puede ejercer una presión excesiva sobre los discos intervertebrales, provocando hernias o degeneraciones con el tiempo.
Es importante señalar que los efectos a largo plazo de la lordosis pueden variar en función de la causa subyacente, la gravedad de la curvatura y factores individuales. El seguimiento periódico y el tratamiento adecuado son esenciales para prevenir o minimizar estas posibles complicaciones.
¿Qué es la escoliosis?
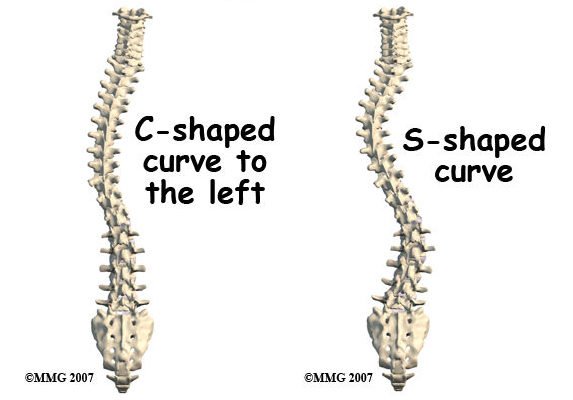
La escoliosis es una enfermedad caracterizada por una curvatura lateral anormal de la columna vertebral. En lugar de que la columna vertebral parezca recta vista de frente o de espaldas, puede tener forma de "S" o de "C". La escoliosis puede afectar a personas de todas las edades, pero es más frecuente que se desarrolle durante la adolescencia.
Causas y factores de riesgo de la escoliosis
La causa exacta de la escoliosis suele ser desconocida y se denomina escoliosis idiopática. Sin embargo, se han identificado ciertos factores de riesgo. Entre ellos están los antecedentes familiares de escoliosis, el sexo femenino (ya que la escoliosis es más frecuente en las niñas), el crecimiento rápido durante la adolescencia y ciertas afecciones neuromusculares como la parálisis cerebral o la distrofia muscular.
Síntomas y diagnóstico de la escoliosis
Los síntomas de la escoliosis pueden variar en función de la gravedad de la curvatura. En los casos leves, puede no haber síntomas perceptibles, mientras que en los casos más graves, las personas pueden experimentar dolor de espalda, rigidez muscular y alturas desiguales de hombros o caderas. En algunos casos, la escoliosis también puede afectar a la postura y el aspecto general del individuo.
Para diagnosticar la escoliosis, un profesional sanitario suele realizar una exploración física, evaluar el historial médico de la persona y puede solicitar pruebas de imagen como radiografías o resonancias magnéticas. Estas pruebas ayudan a determinar el grado de curvatura, identificar las causas subyacentes y orientar las decisiones de tratamiento.
Opciones de tratamiento para la escoliosis
El tratamiento de la escoliosis depende de varios factores, como la gravedad de la curvatura, la edad del individuo y la presencia de cualquier enfermedad subyacente. En los casos leves, puede bastar con un seguimiento regular, sin necesidad de tratamiento específico. Sin embargo, las personas con escoliosis de moderada a grave pueden requerir una intervención para evitar una mayor progresión y controlar los síntomas.
Una opción de tratamiento habitual para la escoliosis es el uso de corsés. Estos corsés están diseñados para ejercer presión sobre la columna vertebral y ayudar a corregir la curvatura. Los corsés suelen recomendarse a personas que aún están creciendo y tienen una curvatura de entre 25 y 45 grados. También puede prescribirse fisioterapia para mejorar la fuerza muscular y la flexibilidad.
En los casos en que la curvatura es grave o progresa rápidamente, puede considerarse la cirugía. La cirugía de fusión espinal es el procedimiento quirúrgico más habitual para la escoliosis. Consiste en fusionar las vértebras mediante varillas metálicas, tornillos o ganchos para enderezar la columna y evitar una mayor curvatura.
Complicaciones y efectos a largo plazo de la escoliosis
Si no se trata, la escoliosis puede provocar diversas complicaciones y efectos a largo plazo. Entre ellos, dolor de espalda crónico, problemas respiratorios por reducción de la capacidad pulmonar, disminución de la movilidad y efectos psicológicos como problemas de autoestima. Además, la escoliosis grave puede ejercer una presión excesiva sobre los discos intervertebrales, provocando hernias o degeneración con el tiempo.
Un seguimiento regular y un tratamiento adecuado son cruciales para prevenir o minimizar estas posibles complicaciones. Es importante señalar que los efectos a largo plazo de la escoliosis pueden variar en función de la gravedad de la curvatura, la edad de aparición y factores individuales.
Conclusión
La lordosis y la escoliosis son dos afecciones distintas de la columna vertebral que implican una curvatura anormal de la columna. Mientras que la lordosis se caracteriza por una curvatura excesiva de la parte inferior de la espalda hacia dentro, la escoliosis implica una curvatura lateral anormal. Comprender las características únicas, las causas, los síntomas, el diagnóstico, las opciones de tratamiento y las posibles complicaciones de cada afección es esencial para un diagnóstico preciso y un tratamiento eficaz.
Tanto la lordosis como la escoliosis pueden tener importantes repercusiones en la calidad de vida de una persona si no se tratan. Por lo tanto, la detección precoz, el tratamiento adecuado y el seguimiento periódico son cruciales para prevenir la progresión, controlar los síntomas y minimizar las posibles complicaciones. Mediante la sensibilización y el fomento de la comprensión de estas afecciones, podemos garantizar que las personas con lordosis o escoliosis reciban la atención y el apoyo que necesitan para llevar una vida sana y satisfactoria.
Referencias
- Smith, J.R., & McCarthy, R.E. "Lordosis y sus implicaciones clínicas". Spine (Phila Pa 1976). 2009;34(10):1050-1057. doi: 10.1097/BRS.0b013e3181a13f6b.
- Weinstein, S.L., Dolan, L.A., Cheng, J.C., Danielsson, A., & Morcuende, J.A. "Escoliosis idiopática del adolescente". The Lancet. 2008;371(9623):1527-1537. doi: 10.1016/S0140-6736(08)60658-3.
- Sato, K., & Kikuchi, S. "Lordosis y sus efectos en la columna vertebral". Clínicas Ortopédicas de Norteamérica. 2011;42(4):543-550. doi: 10.1016/j.ocl.2011.07.002.
- Negrini, S., Donzelli, S., Aulisa, A.G., et al. "2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth". Escoliosis y trastornos de la columna vertebral. 2018;13:3. doi: 10.1186/s13013-017-0145-8.
- Danielsson, A.J., Nachemson, A.L. "Escoliosis infantil y adolescente y el efecto del corsé". Spine (Phila Pa 1976). 2001;26(18):2006-2012. doi: 10.1097/00007632-200109150-00016.
- Balagué, F., Pellisé, F., & Aebi, M. "Escoliosis idiopática". Buenas prácticas e investigación Reumatología clínica. 2007;21(2):227-239. doi: 10.1016/j.berh.2006.12.002.
- Weinstein, S.L., Zavala, D.C., Ponseti, I.V. "Escoliosis idiopática: seguimiento a largo plazo y pronóstico en pacientes no tratados". Revista de cirugía ósea y articular. 1981;63(5):702-712. doi: 10.2106/00004623-198163050-00004.
- Mac-Thiong, J.M., Transfeldt, E.E., Parent, S., Labelle, H. "Corrección quirúrgica de la lordosis en deformidades de la columna vertebral". Spine (Phila Pa 1976). 2012;37(19):1593-1601. doi: 10.1097/BRS.0b013e318251892b.
- Cheng, J.C., Castelein, R.M., Chu, W.C., et al. "Escoliosis idiopática del adolescente". Nature Reviews Cartillas sobre enfermedades. 2015;1:15030. doi: 10.1038/nrdp.2015.30.
- Danielsson, A.J., Hasserius, R., Ohlin, A., Nachemson, A.L. "Escoliosis en el adulto: resultados de la cirugía". Spine (Phila Pa 1976). 2007;32(3):302-310. doi: 10.1097/01.brs.0000254282.30943.8b.
- Reamy, B.V., Slakey, J.B. "Escoliosis idiopática del adolescente: revisión y conceptos actuales". Médico de familia estadounidense. 2001;64(1):111-116. doi: 10.1007/s10437-005-0002-7.
- Weiss, H.R., Lehnert-Schroth, C., Moramarco, M. "El método Schroth de tratamiento de la escoliosis: revisión de la literatura". Estudios de Tecnología e Informática Sanitarias. 2012;176:303-306. doi: 10.3233/978-1-60750-961-7-303.
- Yanik, E.L., Becker, A.C., Lungren, M.P., et al. "MRI assessment of spine deformity in pediatric scoliosis". Revista de Resonancia Magnética. 2021;53(5):1352-1363. doi: 10.1002/jmri.27314.
- Smith, J.S., Klineberg, E., Schwab, F.J., et al. "Prospective multicenter assessment of perioperative and minimum 2-year postoperative complication rates associated with adult spinal deformity surgery". Revista de Neurocirugía: Spine. 2017;26(6):730-740. doi: 10.3171/2016.10.SPINE16334.
- Bunnell, W.P. "La historia natural de la escoliosis idiopática antes de la madurez esquelética". Spine (Phila Pa 1976). 1986;11(8):773-776. doi: 10.1097/00007632-198610000-00006.