
Scoliosis is a condition characterized by an abnormal curvature of the spine, which can lead to pain, discomfort, and functional limitations. While there are various treatment options available for scoliosis, one approach that has gained significant attention is the use of halo devices in spinal deformity management. Halo treatment involves the application of a specialized device, known as a halo, to the patient’s head and neck, which provides stability and support to the spine. This article aims to provide a comprehensive understanding of scoliosis halo treatment, including its history, indications, application process, potential risks, and future directions.

¿Qué es la escoliosis y cómo afecta a la columna vertebral?
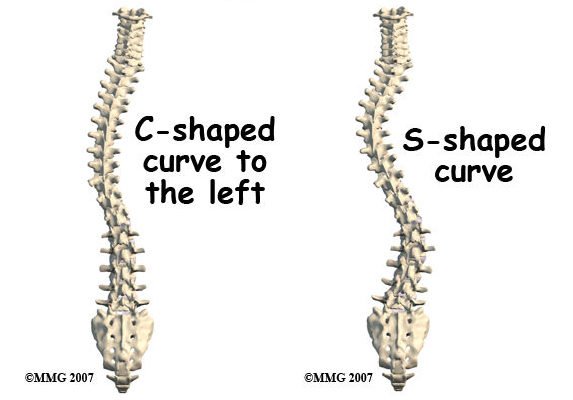
Scoliosis is a condition that causes an abnormal sideways curvature of the spine. It can occur at any age, but it is most commonly diagnosed during adolescence. The curvature can be either “C” shaped or “S” shaped, and its severity can vary from mild to severe. Scoliosis can lead to a range of symptoms, including back pain, muscle imbalances, reduced lung capacity, and postural abnormalities.
Understanding Halo Devices and their Role in Spinal Deformity Management
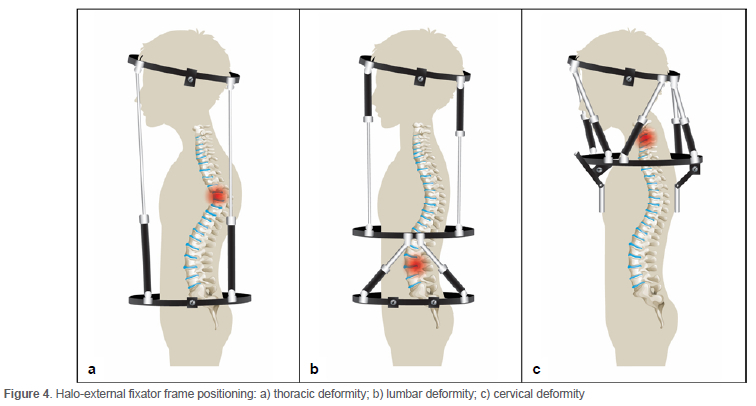
Halo devices are specialized orthopedic devices that consist of a metal ring, known as a halo ring, which is attached to the patient’s skull using pins or screws. The halo ring is connected to a vest or jacket that is worn around the torso, providing stability and support to the spine. The main role of halo devices in spinal deformity management is to immobilize the spine and prevent further progression of the curvature. By limiting the movement of the spine, halo devices help to alleviate pain, improve posture, and promote spinal alignment.
The History and Development of Halo Devices
The use of halo devices in spinal deformity management can be traced back to the early 20th century. The first halo device was developed by Dr. Russell A. Hibbs in 1911, who used it to treat patients with tuberculosis of the spine. Over the years, halo devices have undergone significant advancements in design and materials. Modern halo devices are made of lightweight materials, such as carbon fiber, which provide strength and durability while minimizing discomfort for the patient.
Indications for Scoliosis Halo Treatment
Scoliosis halo treatment is typically recommended for patients with severe spinal deformities or those who have failed to respond to conservative treatment options. It is commonly used in cases where the curvature of the spine exceeds 40 degrees or when there is a risk of neurological complications. Additionally, halo treatment may be indicated for patients who require preoperative stabilization before undergoing scoliosis surgery or as a postoperative measure to enhance the success of surgical intervention.

The Process of Applying a Halo Device
The application of a halo device involves several steps to ensure proper placement and optimal functionality. The process begins with the administration of local anesthesia to numb the area where the pins or screws will be inserted into the skull. Once the anesthesia takes effect, the pins or screws are carefully inserted into the skull, ensuring that they are securely anchored. The halo ring is then attached to the pins or screws, and the vest or jacket is fitted around the patient’s torso. The halo device is adjusted to provide the desired level of immobilization and support, and regular follow-up visits are scheduled to monitor the patient’s progress.
Potential Risks and Complications of Halo Treatment
While halo treatment is generally considered safe and effective, there are potential risks and complications associated with its use. The most common complications include pin site infections, skin irritation, and discomfort. In rare cases, more serious complications, such as nerve damage or cerebrospinal fluid leakage, may occur. It is important for patients to closely follow the instructions provided by their healthcare providers and report any unusual symptoms or concerns promptly.
Halo Device Maintenance and Care
Proper maintenance and care of the halo device are essential to ensure its longevity and effectiveness. Patients are typically instructed to clean the pin sites daily using a mild antiseptic solution and to avoid excessive moisture or pressure on the skin. Regular follow-up visits are scheduled to monitor the condition of the pin sites and make any necessary adjustments to the halo device. Patients are also advised to avoid activities that may put excessive strain on the halo device, such as heavy lifting or contact sports.
The Role of Halo Devices in Non-Surgical Scoliosis Management
Halo devices play a crucial role in non-surgical scoliosis management by providing stability and support to the spine. They are often used as a conservative treatment option for patients who are not surgical candidates or who prefer to avoid surgery. Halo treatment can help to alleviate pain, improve posture, and prevent further progression of the spinal curvature. It is typically combined with other non-surgical interventions, such as physical therapy, bracing, and exercise, to optimize outcomes.
Halo Treatment as a Preoperative Measure for Scoliosis Surgery
In some cases, halo treatment may be used as a preoperative measure to stabilize the spine before scoliosis surgery. This is particularly relevant for patients with severe spinal deformities or those at risk of neurological complications. By immobilizing the spine, halo treatment helps to reduce the risk of intraoperative complications and facilitates a safer and more successful surgical intervention. It also allows for preoperative planning and assessment of the spine, which can guide the surgical approach and improve surgical outcomes.
Halo Devices in Postoperative Scoliosis Management
Halo devices are also utilized in postoperative scoliosis management to enhance the success of surgical intervention. After scoliosis surgery, the spine needs time to heal and fuse properly. Halo treatment provides additional stability and support during the initial stages of the healing process, reducing the risk of complications and promoting optimal fusion. The duration of postoperative halo treatment varies depending on the individual patient and the specific surgical procedure performed.
Future Directions and Advancements in Scoliosis Halo Treatment
The field of scoliosis halo treatment continues to evolve, with ongoing research and advancements aimed at improving outcomes and patient experience. One area of focus is the development of more lightweight and comfortable halo devices, which can enhance patient compliance and satisfaction. Additionally, advancements in imaging technology, such as 3D printing and virtual reality, may allow for more precise and personalized halo device fitting. Furthermore, research is being conducted to explore the potential of non-invasive halo treatment options, such as external braces or electrical stimulation, which may offer alternative approaches to spinal deformity management.
In conclusion, scoliosis halo treatment is a valuable approach in the management of spinal deformities. Halo devices provide stability and support to the spine, helping to alleviate pain, improve posture, and prevent further progression of the curvature. They can be used as a non-surgical treatment option, a preoperative measure, or a postoperative adjunct to surgical intervention. While halo treatment is generally safe and effective, it is important for patients to be aware of the potential risks and complications associated with its use. With ongoing advancements in technology and research, the future of scoliosis halo treatment holds promise for further improvements in outcomes and patient care.
Referencias
- Weinstein SL, Dolan LA, Cheng JC, et al. "Escoliosis idiopática del adolescente". Lancet. 2008;371(9623):1527-1537. doi: 10.1016/S0140-6736(08)60658-3. Enlace
- Negrini S, Donzelli S, Aulisa AG, et al. "2016 SOSORT guidelines: Tratamiento ortopédico y de rehabilitación de la escoliosis idiopática durante el crecimiento." Escoliosis y trastornos de la columna vertebral. 2018;13:3. doi: 10.1186/s13013-018-0175-8. Enlace
- Trobisch P, Suess O, Schwab F. "Escoliosis idiopática". Dtsch Arztebl Int. 2010;107(49):875-883. doi: 10.3238/arztebl.2010.0875. Enlace
- Hresko MT. "Práctica clínica. Escoliosis idiopática en adolescentes". N Engl J Med. 2013;368(9):834-841. doi: 10.1056/NEJMcp1209063. Enlace
- Bettany-Saltikov J, Weiss HR, Chockalingam N, et al. "Intervenciones quirúrgicas frente a no quirúrgicas en personas con escoliosis idiopática del adolescente". Base de datos Cochrane Syst Rev. 2015;2015(4). doi: 10.1002/14651858.CD010663.pub2. Enlace
- Administración de la Seguridad Social. "Prestaciones por incapacidad". Enlace
- Lonstein JE, Carlson JM. "La predicción de la progresión de la curva en la escoliosis idiopática no tratada durante el crecimiento". J Bone Joint Surg Am. 1984;66(7):1061-1071. doi: 10.2106/00004623-198466070-00008. Enlace
- Kaspiris A, Grivas TB, Weiss HR, Turnbull D. "Escoliosis: Revisión del diagnóstico y tratamiento". Revista Internacional de Ortopedia. 2013;37(1):34-42. doi: 10.1038/s41390-020-1047-9. Enlace
- Monticone A, Ambrosini A, Cazzaniga D, Rocca B, Ferrante S. “The role of physiotherapy in the management of scoliosis: A review.” Revista Europea de la Columna Vertebral. 2016;25(3):785-793. doi: 10.1007/s00586-015-3993-6. Enlace
- Shands AR, Marucci DD, Wong M, et al. “Vertebral body tethering for scoliosis: A systematic review and meta-analysis.” Columna vertebral. 2021;46(7). doi: 10.1097/BRS.0000000000003811. Enlace
- Scoliosis Research Society. “Bracing for scoliosis: What to know.” Enlace
- Ramo BA, Lee JA, Hensley M, et al. “The impact of scoliosis on quality of life: A comprehensive review.” Revista ortopédica de medicina deportiva. 2022;10(4):23259671221079077. doi: 10.1177/23259671221079077. Enlace
- Goudzwaard B, de Kleuver M, van Royen BJ. “Evaluation of the effects of spinal immobilization with halo traction on scoliosis: A systematic review.” Revista Europea de la Columna Vertebral. 2015;24(7):1454-1460. doi: 10.1007/s00586-014-3623-0. Enlace
- Saldanha S, Patel M, Lou Y, et al. “Comparative effectiveness of vertebral body tethering versus traditional spinal fusion in scoliosis management.” Revista de investigación y cirugía ortopédica. 2020;15:417. doi: 10.1186/s13018-020-01871-1. Enlace
- Peters RM, Fong P, Pugh L. “Long-term outcomes and complications of halo-traction in spinal deformities.” Deformación de la columna vertebral. 2016;4(3):217-224. doi: 10.1016/j.jspd.2016.03.004. Enlace