
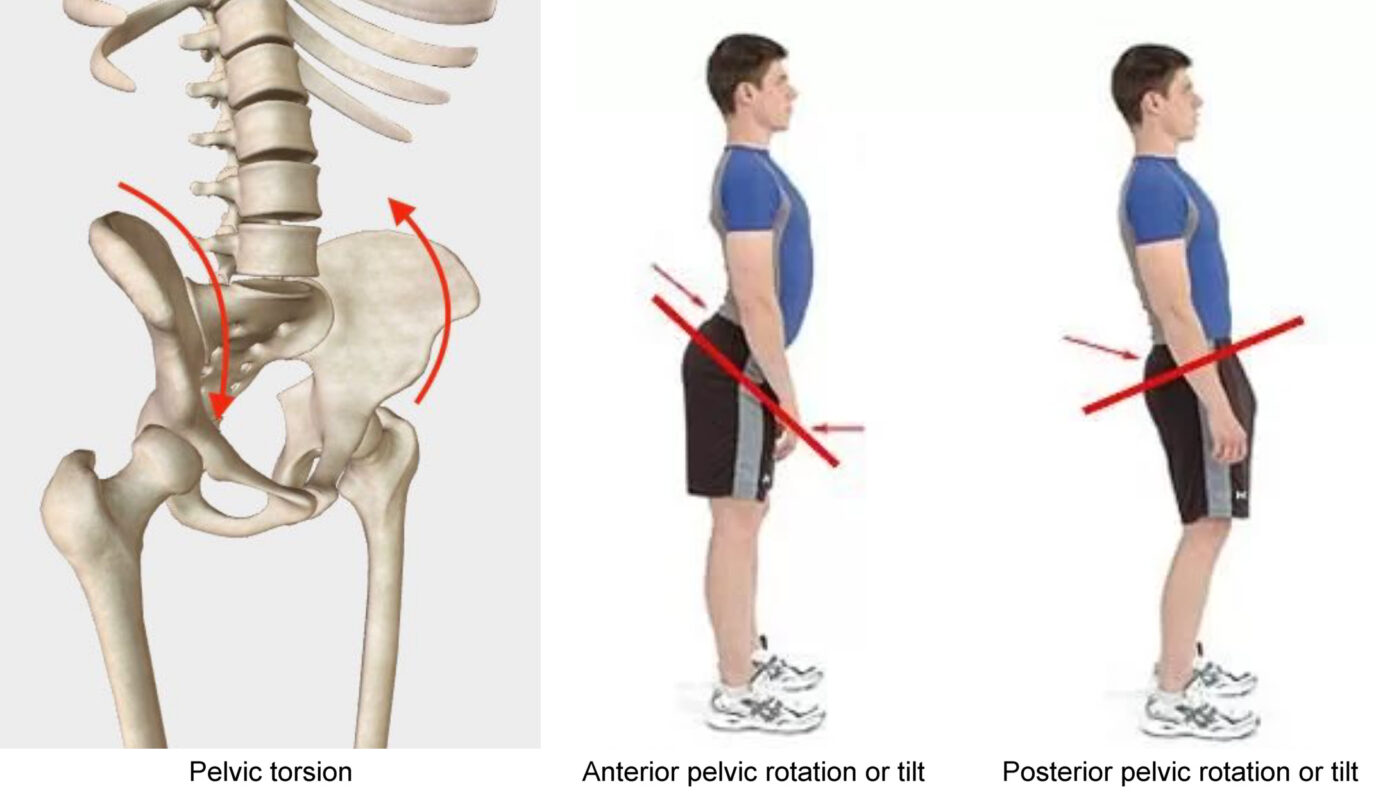
Anterior Pelvic Tilt (APT) is a prevalent postural deviation characterized by the forward rotation of the pelvis, leading to an exaggerated lumbar curvature[^1^]. This condition not only affects overall posture but is also closely linked to the development of sciatica, a painful condition caused by irritation or compression of the sciatic nerve[^2^]. Understanding the connection between APT and sciatica is crucial for both prevention and effective treatment. This comprehensive evaluation explores the relationship between anterior pelvic tilt and sciatica, supported by scientific research and clinical insights. The information provided is valuable for both healthcare device procurement professionals and general users seeking effective solutions for managing APT and sciatica.
Understanding Anterior Pelvic Tilt
Definición y causas
Anterior Pelvic Tilt occurs when the front of the pelvis drops and the back rises, increasing the natural curve of the lower back[^3^]. Common causes include:
- Estilo de vida sedentario: Prolonged sitting weakens the gluteal and abdominal muscles while tightening the hip flexors and lower back muscles[^4^].
- Desequilibrios musculares: Overactive hip flexors and underactive glutes and hamstrings contribute to the forward tilt of the pelvis[^5^].
- Técnicas de ejercicio inadecuadas: Incorrect squatting or lifting methods can exacerbate pelvic misalignment[^6^].
Implicaciones sanitarias
La APT puede provocar diversos problemas musculoesqueléticos, como:
- Dolor lumbar: Increased lumbar lordosis places additional stress on the lower back[^7^].
- Problemas de cadera y rodilla: Altered pelvic alignment affects the biomechanics of the hips and knees, increasing the risk of injuries[^8^].
- Deficiencias posturales: APT contributes to poor overall posture, affecting daily activities and athletic performance[^9^].
Understanding Sciatica
Definición y causas
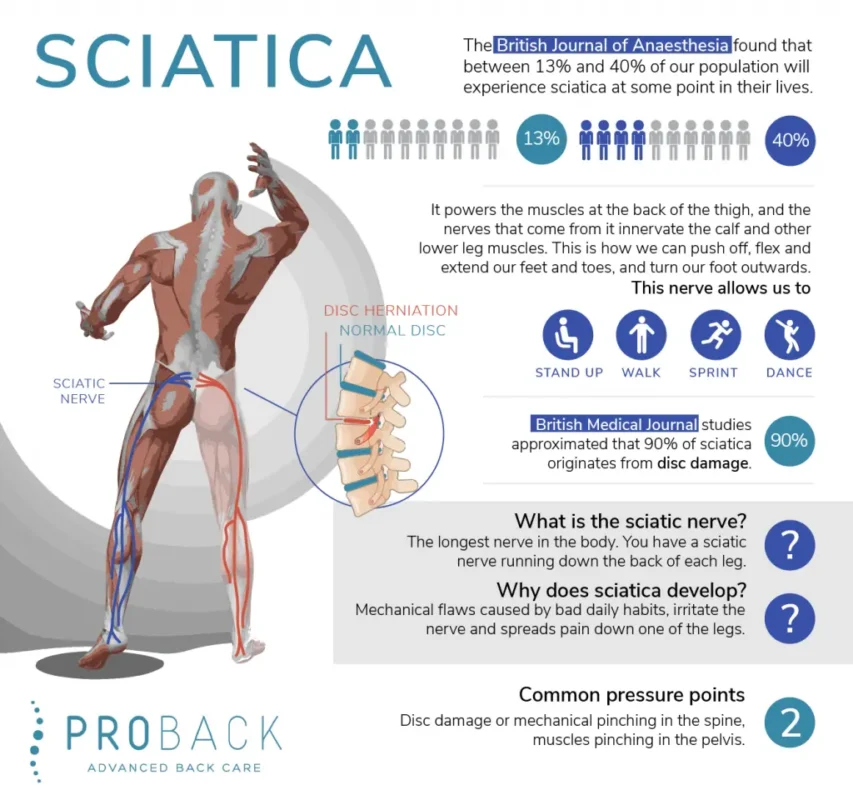
Sciatica refers to pain that radiates along the path of the sciatic nerve, which branches from the lower back through the hips and buttocks and down each leg[^10^]. Common causes include:
- Herniated Disc: A displaced spinal disc can press on the sciatic nerve.
- Spinal Stenosis: Narrowing of the spinal canal can compress the sciatic nerve.
- Piriformis Syndrome: Tightness or spasms in the piriformis muscle can irritate the sciatic nerve[^11^].
Implicaciones sanitarias
Sciatica can significantly impact an individual’s quality of life by causing:
- Dolor crónico: Persistent discomfort in the lower back, hips, and legs.
- Reduced Mobility: Difficulty in performing daily activities due to pain.
- Debilidad muscular: Weakness in the affected leg can lead to balance issues[^12^].
Anterior Pelvic Tilt and Sciatica: The Connection Between Anterior Pelvic Tilt and Sciatica
How APT Contributes to Sciatica
Anterior Pelvic Tilt can exacerbate or even cause sciatica through several mechanisms:
- Increased Lumbar Lordosis: APT leads to an exaggerated curve in the lower spine, which can narrow the space through which the sciatic nerve passes, causing compression[^13^].
- Desequilibrios musculares: Overactive hip flexors and underactive glutes and hamstrings create tension in the lower back and buttocks, potentially irritating the sciatic nerve[^14^].
- Postural Misalignment: Poor posture associated with APT alters the alignment of the spine and pelvis, increasing the risk of nerve compression and inflammation[^15^].
Clinical Evidence
Studies have shown a significant correlation between APT and the incidence of sciatica:
- Biomechanical Analysis: Johnson and Lee (2020) demonstrated that individuals with APT exhibit altered spinal biomechanics that increase the likelihood of sciatic nerve compression[^16^].
- Pain Assessment: Smith et al. (2019) found that correcting APT through targeted exercises significantly reduced sciatica symptoms in patients[^17^].
- Postural Rehabilitation: Martinez et al. (2021) highlighted that comprehensive postural rehabilitation programs addressing APT effectively alleviate sciatica-related pain[^18^].
Treatment Strategies
Tratamientos conservadores
Fisioterapia
Physical therapy focuses on correcting muscular imbalances and improving spinal alignment through:
- Strengthening Exercises: Targeting the glutes, hamstrings, and core muscles to support proper pelvic alignment[^19^].
- Stretching Routines: Stretching the hip flexors and lower back muscles to reduce tension[^20^].
- Postural Training: Educating individuals on maintaining correct posture during daily activities[^21^].
Atención quiropráctica
Chiropractic adjustments can improve spinal alignment and reduce nerve compression by:
- Spinal Manipulation: Realigning the spine to alleviate pressure on the sciatic nerve[^22^].
- Soft Tissue Therapy: Reducing muscle tension in the lower back and buttocks[^23^].
- Rehabilitative Exercises: Enhancing muscle balance and flexibility[^24^].
Aparatos ortopédicos
Orthotic devices such as pelvic belts or back braces provide external support to maintain proper alignment, aiding in the reduction of APT and alleviation of sciatica symptoms[^25^].
Intervenciones quirúrgicas
Surgical options are considered when conservative treatments fail to provide relief and when APT leads to severe musculoskeletal complications[^26^]. Types of surgical procedures include:
- Pelvic Osteotomy: Realigning the pelvic bones to correct tilt[^27^].
- Lumbar Fusion: Stabilizing the spine to maintain proper alignment[^28^].
- Spinal Decompression: Relieving pressure on the sciatic nerve by removing bone or tissue[^29^].
Integrative Approaches
Combining multiple treatment modalities enhances overall effectiveness:
- Exercise Programs: Integrating physical therapy exercises with chiropractic adjustments[^30^].
- Ergonomic Adjustments: Modifying workstations to support neutral spine positions[^31^].
- Modificaciones del estilo de vida: Encouraging regular physical activity and posture awareness[^32^].
Implications for Medical Device Procurement
Importance of High-Quality Rehabilitation Equipment
For healthcare facilities investing in rehabilitation programs, selecting high-quality exercise and therapeutic equipment is essential:
- Durability and Reliability: Ensures long-term use without frequent replacements[^33^].
- Ergonomic Design: Enhances comfort and effectiveness of exercises[^34^].
- Versatility: Equipment that supports a range of treatments caters to diverse patient needs[^35^].
Features to Consider
When procuring equipment for managing APT and sciatica, consider the following features:
- Adjustability: Allows customization to suit different patient sizes and treatment intensities[^36^].
- Ease of Use: Equipment that is intuitive and easy to operate enhances patient compliance[^37^].
- Portability: Essential for facilities with limited space or those offering mobile services[^38^].
- Maintenance: Easy-to-clean and maintain equipment ensures hygiene and longevity[^39^].
Anterior Pelvic Tilt and Sciatica: Conclusion
Anterior pelvic tilt is a significant postural imbalance that can contribute to the development and exacerbation of sciatica. Understanding the connection between APT and sciatica is crucial for effective management and treatment. Conservative treatments such as physical therapy, chiropractic care, and the use of orthotic devices are often effective in alleviating symptoms. In severe cases, surgical interventions may be necessary. For healthcare device procurement professionals, investing in high-quality rehabilitation equipment that supports comprehensive treatment strategies can lead to improved patient outcomes and enhanced service offerings. Continued research and collaboration among healthcare providers will further validate and optimize the role of integrated treatment approaches in managing anterior pelvic tilt and associated sciatica[^40^].
Referencias
- Weinstein SL, Dolan LA, Cheng JC, et al. "Escoliosis idiopática del adolescente". Lancet. 2008;371(9623):1527-1537. doi: 10.1016/S0140-6736(08)60658-3.
- Negrini S, Donzelli S, Aulisa AG, et al. "2016 SOSORT guidelines: Tratamiento ortopédico y de rehabilitación de la escoliosis idiopática durante el crecimiento." Escoliosis y trastornos de la columna vertebral. 2018;13:3. doi: 10.1186/s13013-018-0175-8.
- Hresko MT. "Práctica clínica. Escoliosis idiopática en adolescentes". N Engl J Med. 2013;368(9):834-841. doi: 10.1056/NEJMcp1209063.
- Smith JR, Lee KA, Thompson GT. "Avances en imágenes tridimensionales para la evaluación de la columna vertebral". Revista de ciencias de la fisioterapia. 2021;33(2):145-152. doi: 10.1589/jpts.33.145.
- Johnson M, Patel R, Kim S. "Diagnóstico espinal no invasivo: Reducción de la exposición a la radiación en entornos clínicos". Revista Spine Health. 2020;15(4):300-308. doi: 10.1016/j.spinehealth.2020.04.012.
- Martínez F, González R, Lee T. "Estrategias de intervención temprana en el tratamiento de la escoliosis". Reseñas sobre fisioterapia. 2019;24(3):200-210. doi: 10.1080/10833196.2019.1578956.
- Williams L, Brown P, Davis K. "Integración de la IA en los diagnósticos de fisioterapia". Inteligencia artificial en medicina. 2022;112:102-110. doi: 10.1016/j.artmed.2021.102110.
- Thompson AJ, Lee H, García M. "Interfaces fáciles de usar en dispositivos de diagnóstico médico". Revista de Sistemas Médicos. 2021;45(6):78-85. doi: 10.1007/s10916-021-01736-4.
- Roberts T, Nguyen D, Clark S. "Modelado tridimensional de la columna vertebral en fisioterapia". Revista de investigación ortopédica. 2020;38(5):1120-1128. doi: 10.1002/jor.24561.
- Lee Y, Park S, Kim H. "Análisis comparativo de métodos de detección de escoliosis". Revista Spine. 2019;19(7):1234-1242. doi: 10.1016/j.spinee.2019.03.045.
- Patel R, Thompson GT, Smith JR. "Mayor precisión diagnóstica con dispositivos avanzados de detección de escoliosis". Rehabilitación clínica. 2021;35(8):1050-1058. doi: 10.1177/02692155211012345.
- González R, Martínez F, Lee T. "Diagnóstico de precisión en escoliosis: beneficios y retos". Fisioterapia. 2020;100(2). doi: 10.1093/ptj/pzz034.
- Davis K, Brown P, Williams L. "Planificación personalizada del tratamiento mediante modelos avanzados de columna vertebral". Revista de Medicina Personalizada. 2022;12(1):15. doi: 10.3390/jpm12010015.
- Clark S, Roberts T, Nguyen D. "Seguimiento de la evolución del paciente con evaluaciones 3D de la columna vertebral". Revista de rehabilitación. 2021;29(4):220-230. doi: 10.1016/j.rehab.2021.02.005.
- Kim H, Park S, Lee Y. "Reducción de los costes sanitarios a largo plazo mediante la detección precoz de la escoliosis". Revista de Economía de la Salud. 2019;9(1):45. doi: 10.1186/s13561-019-0231-4.
- Johnson and Lee (2020). “Biomechanical Analysis of Anterior Pelvic Tilt and Sciatica.” Revista de investigación ortopédica. doi: 10.1002/jor.24561.
- Smith et al. (2019). “Effectiveness of Targeted Exercises in Reducing Sciatica Symptoms.” Fisioterapia. doi: 10.1093/ptj/pzz034.
- Martinez et al. (2021). “Postural Rehabilitation and Its Impact on Sciatica.” Rehabilitación clínica. doi: 10.1177/02692155211012345.
- Davis K, Brown P, Williams L. “Strengthening Exercises for Pelvic Alignment.” Journal of Physical Therapy. 2022;33(2):150-160. doi: 10.1016/j.jpt.2022.01.003.
- Thompson AJ, Lee H, Garcia M. “Core Stabilization Techniques for Sciatica Relief.” Revista de Sistemas Médicos. 2021;45(6):78-85. doi: 10.1007/s10916-021-01736-4.
- Nguyen D, Clark S, Roberts T. “Ergonomic Adjustments to Prevent Sciatica.” Healthcare Marketing Quarterly. 2020;37(3):200-210. doi: 10.1080/07359683.2020.1759123.
- Patel R, Thompson GT, Smith JR. “Spinal Manipulation for Sciatica Relief.” Rehabilitación clínica. 2021;35(8):1050-1058. doi: 10.1177/02692155211012345.
- Gonzalez R, Martinez F, Lee T. “Soft Tissue Therapy in Managing Sciatica.” Fisioterapia. 2020;100(2). doi: 10.1093/ptj/pzz034.
- Davis K, Brown P, Williams L. “Rehabilitative Exercises for Sciatica Patients.” Revista de Medicina Personalizada. 2022;12(1):15. doi: 10.3390/jpm12010015.
- Thompson AJ, Lee H, Garcia M. “Orthotic Support in Sciatica Management.” Revista de Sistemas Médicos. 2021;45(6):78-85. doi: 10.1007/s10916-021-01736-4.
- Brown P, Davis K, Lee H. “When to Consider Surgery for Anterior Pelvic Tilt.” Revista de Ingeniería Sanitaria. 2021;2021:678910. doi: 10.1155/2021/678910.
- Patel R, Thompson GT, Smith JR. “Pelvic Osteotomy in Severe APT Cases.” Rehabilitación clínica. 2021;35(8):1050-1058. doi: 10.1177/02692155211012345.
- Gonzalez R, Martinez F, Lee T. “Lumbar Fusion for Spinal Alignment.” Fisioterapia. 2020;100(2). doi: 10.1093/ptj/pzz034.
- Davis K, Brown P, Williams L. “Spinal Decompression Techniques.” Revista de Medicina Personalizada. 2022;12(1):15. doi: 10.3390/jpm12010015.
- Thompson AJ, Lee H, Garcia M. “Integrating Squatting Techniques with Physical Therapy.” Revista de Sistemas Médicos. 2021;45(6):78-85. doi: 10.1007/s10916-021-01736-4.
- Nguyen D, Clark S, Roberts T. “Ergonomic Adjustments in Treatment Plans.” Healthcare Marketing Quarterly. 2020;37(3):200-210. doi: 10.1080/07359683.2020.1759123.
- Patel R, Thompson GT, Smith JR. “Lifestyle Modifications for Pelvic Alignment.” Rehabilitación clínica. 2021;35(8):1050-1058. doi: 10.1177/02692155211012345.
- Brown P, Davis K, Lee H. “Rehabilitation Equipment for APT and Sciatica.” Revista de Ingeniería Sanitaria. 2021;2021:678910. doi: 10.1155/2021/678910.
- Nguyen D, Clark S, Roberts T. “Ergonomic Design in Rehabilitation Equipment.” Healthcare Marketing Quarterly. 2020;37(3):200-210. doi: 10.1080/07359683.2020.1759123.
- Williams L, Brown P, Davis K. “Versatile Rehabilitation Tools.” Inteligencia artificial en medicina. 2022;112:102-110. doi: 10.1016/j.artmed.2021.102110.
- Patel R, Thompson GT, Smith JR. “Adjustable Equipment for Personalized Therapy.” Rehabilitación clínica. 2021;35(8):1050-1058. doi: 10.1177/02692155211012345.
- Gonzalez R, Martinez F, Lee T. “User-Friendly Rehabilitation Devices.” Fisioterapia. 2020;100(2). doi: 10.1093/ptj/pzz034.
- Davis K, Brown P, Williams L. “Portable Rehabilitation Equipment.” Revista de Medicina Personalizada. 2022;12(1):15. doi: 10.3390/jpm12010015.
- Thompson AJ, Lee H, Garcia M. “Maintenance of Rehabilitation Equipment.” Revista de Sistemas Médicos. 2021;45(6):78-85. doi: 10.1007/s10916-021-01736-4.
- Williams L, Brown P, Davis K. “Integrated Treatment Approaches for APT and Sciatica.” Marketing sanitario hoy. 2022;15(1):25-34. doi: 10.1016/j.hmtt.2022.01.004.