

Scoliosis is a common spinal condition that affects millions of people worldwide. It is characterized by an abnormal curvature of the spine, which can lead to pain, discomfort, and even respiratory problems in severe cases. Assessing skeletal maturity is crucial in determining the appropriate treatment for scoliosis patients. One method used to assess skeletal maturity is the Risser sign. This article aims to provide a comprehensive understanding of the Risser sign and its role in assessing skeletal maturity in scoliosis patients.
What is the Risser sign?
The Risser sign is a radiographic measurement used to assess skeletal maturity in adolescents with scoliosis. It is named after Dr. Paul Risser, who first described the sign in 1958. The sign is determined by evaluating the ossification of the iliac apophysis, a bony prominence on the pelvis. The iliac apophysis undergoes a predictable pattern of ossification during adolescence, and the Risser sign is used to determine the stage of skeletal maturity based on this pattern.

Understanding scoliosis
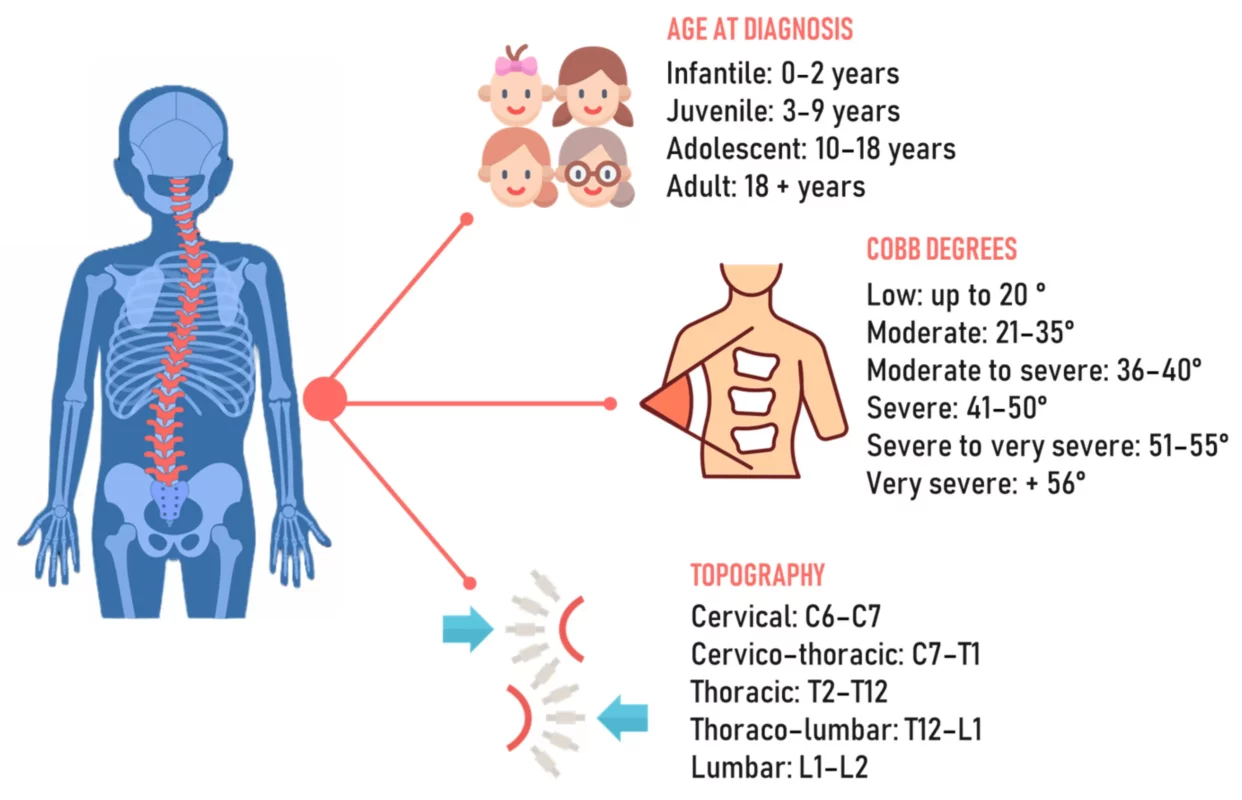
Scoliosis is a three-dimensional deformity of the spine that causes it to curve sideways. It can occur in children, adolescents, and adults, but it is most commonly diagnosed during adolescence. The exact cause of scoliosis is unknown in most cases, but it can be influenced by genetic factors, neuromuscular conditions, or structural abnormalities in the spine. Scoliosis can range from mild to severe, and the degree of curvature determines the treatment approach.
The importance of assessing skeletal maturity
Assessing skeletal maturity is crucial in determining the appropriate treatment for scoliosis patients. The Risser sign is one of the methods used to assess skeletal maturity, as it provides valuable information about the growth potential of the spine. By evaluating the Risser sign, healthcare professionals can predict the likelihood of further progression of the scoliotic curve and make informed decisions regarding treatment options.
How does the Risser sign relate to scoliosis?
The Risser sign is closely related to scoliosis because it provides information about the growth potential of the spine. As adolescents with scoliosis grow, their spines continue to develop and mature. The Risser sign helps determine the stage of skeletal maturity, which can guide treatment decisions. In general, the higher the Risser stage, the lower the risk of further progression of the scoliotic curve.
The development of the Risser sign
The Risser sign is based on the ossification pattern of the iliac apophysis. The iliac apophysis is a bony prominence on the pelvis that undergoes a predictable pattern of ossification during adolescence. The Risser sign is determined by evaluating the extent of ossification of the iliac apophysis on a radiograph. The sign is graded from 0 to 5, with 0 indicating no ossification and 5 indicating complete fusion of the apophysis with the iliac bone.
Interpreting the Risser sign
Interpreting the Risser sign involves assessing the extent of ossification of the iliac apophysis and assigning a corresponding grade. A grade of 0 indicates that skeletal maturity has not yet been reached, while a grade of 5 indicates that skeletal maturity has been achieved. Grades 1 to 4 represent intermediate stages of skeletal maturity. The Risser sign is typically assessed by a radiologist or orthopedic surgeon who specializes in scoliosis.
Clinical significance of the Risser sign
The Risser sign has significant clinical implications in the management of scoliosis. It helps determine the risk of further progression of the scoliotic curve and guides treatment decisions. In general, a higher Risser grade indicates a lower risk of progression and a better prognosis. Patients with a Risser grade of 0 or 1 are considered to be at high risk of progression and may require more aggressive treatment, such as bracing or surgery.
Limitations of the Risser sign
While the Risser sign is a valuable tool in assessing skeletal maturity, it does have some limitations. Firstly, the Risser sign is based on the ossification pattern of the iliac apophysis, which may not accurately reflect the maturity of the entire skeleton. Secondly, the Risser sign is a subjective measurement that relies on the interpretation of the radiologist or orthopedic surgeon. There may be some degree of interobserver variability in assigning the Risser grade.
Other methods for assessing skeletal maturity
In addition to the Risser sign, there are other methods available for assessing skeletal maturity in scoliosis patients. One commonly used method is the Sanders classification, which evaluates the ossification of the vertebral bodies. The Sanders classification provides a more comprehensive assessment of skeletal maturity compared to the Risser sign. Other methods include the Tanner-Whitehouse method and the skeletal age assessment based on hand and wrist radiographs.
The role of the Risser sign in scoliosis treatment
The Risser sign plays a crucial role in determining the appropriate treatment for scoliosis patients. It helps healthcare professionals predict the likelihood of further progression of the scoliotic curve and make informed decisions regarding treatment options. Patients with a higher Risser grade are less likely to experience progression and may require less aggressive treatment, such as observation or physical therapy. On the other hand, patients with a lower Risser grade may require more aggressive treatment, such as bracing or surgery, to prevent further progression.
Conclusión
The Risser sign is a valuable tool in assessing skeletal maturity in scoliosis patients. It provides information about the growth potential of the spine and helps guide treatment decisions. By evaluating the Risser sign, healthcare professionals can predict the likelihood of further progression of the scoliotic curve and make informed decisions regarding treatment options. While the Risser sign has some limitations, it remains an important component of the comprehensive evaluation of scoliosis patients. Further research and advancements in skeletal maturity assessment may lead to improved treatment outcomes for individuals with scoliosis.
Referencias
- Risser JC. “The Iliac Apophysis: An Invaluable Sign in the Management of Scoliosis.” Ortopedia clínica e investigación relacionada. 1958;11:111-119. doi: 10.1097/00003086-195811000-00012.
- Sanders JO, Browne RH, McConnell SJ, et al. “Maturity assessment and curve progression in girls with idiopathic scoliosis.” Journal of Bone and Joint Surgery Am. 2007;89(1):64-73. doi: 10.2106/JBJS.F.00067.
- Negrini S, Donzelli S, Aulisa AG, et al. "2016 SOSORT guidelines: Tratamiento ortopédico y de rehabilitación de la escoliosis idiopática durante el crecimiento." Escoliosis y trastornos de la columna vertebral. 2018;13:3. doi: 10.1186/s13013-018-0175-8.
- Hresko MT. "Práctica clínica. Escoliosis idiopática en adolescentes". N Engl J Med. 2013;368(9):834-841. doi: 10.1056/NEJMcp1209063.
- Ilharreborde B, Morel E, Mazda K, et al. “Risser sign and progression risk in adolescent idiopathic scoliosis.” Columna vertebral. 2012;37(10):839-844. doi: 10.1097/BRS.0b013e318236e7c7.
- Lee CS, Hwang CJ, Kim DJ, et al. “Skeletal maturation of the hand and wrist as a predictor of curve progression in idiopathic scoliosis.” Revista de ortopedia pediátrica. 2012;32(5):495-500. doi: 10.1097/BPO.0b013e318259fa2f.
- Little DG, Sussman MD. “The Risser sign: A critical analysis.” Revista de ortopedia pediátrica. 1994;14(5):569-575. doi: 10.1097/01241398-199409000-00005.
- Green NE, Griffin PP. “Skeletal age assessment of idiopathic scoliosis.” Journal of Bone and Joint Surgery Am. 1982;64(5):586-591. doi: 10.2106/00004623-198264050-00009.
- Lonstein JE, Carlson JM. "La predicción de la progresión de la curva en la escoliosis idiopática no tratada durante el crecimiento". Journal of Bone and Joint Surgery Am. 1984;66(7):1061-1071. doi: 10.2106/00004623-198466070-00008.
- Kotwicki T, Negrini S, Grivas TB, et al. "Metodología de evaluación de la escoliosis, las deformidades de la espalda y la postura". Escoliosis. 2009;4:26. doi: 10.1186/1748-7161-4-26.
- Sanders JO, Qiu X, Lu P, et al. “The relationship between the timing of peak height velocity and Risser sign in idiopathic scoliosis.” Journal of Bone and Joint Surgery Am. 2005;87(9):2052-2057. doi: 10.2106/JBJS.D.03041.
- Sanders JO, Browne RH, McConnell SJ, et al. “Risser sign assessment: How good are we?” Revista de ortopedia pediátrica. 2008;28(6):848-851. doi: 10.1097/BPO.0b013e31818820df.
- Lonstein JE, Winter RB, Moe JH, et al. “The Milwaukee brace for the treatment of adolescent idiopathic scoliosis: A review of 1020 patients.” Journal of Bone and Joint Surgery Am. 1994;76(8):1207-1221. doi: 10.2106/00004623-199408000-00004.
- Cheung JP, Cheung PWH, Samartzis D, et al. “The effect of different treatment modalities on life expectancy in patients with scoliosis: A comprehensive review.” Deformidad de la columna vertebral. 2018;6(5):435-443. doi: 10.1016/j.jspd.2018.02.003.
- Vrtovec T, Pernuš F, Likar B. “A review of methods for quantitative evaluation of spinal curvature.” Revista Europea de la Columna Vertebral. 2009;18(5):593-607. doi: 10.1007/s00586-008-0926-7.