
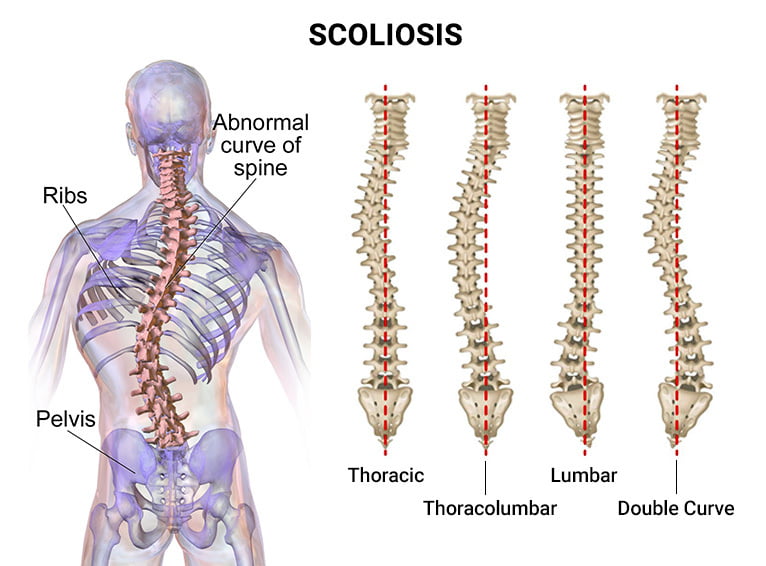
Scoliosis is a complex spinal condition characterized by an abnormal curvature of the spine. It affects approximately 2-3% of the population, with the majority of cases occurring in adolescents. Understanding the anatomy of scoliosis is crucial for comprehending the structural changes that occur and their implications for function and health.
The Spinal Column: A Complex Structure
The spinal column, also known as the vertebral column or backbone, is a complex structure consisting of 33 vertebrae. It serves as the main support for the body, protecting the spinal cord and allowing for movement. In scoliosis, the normal alignment of the vertebrae is disrupted, resulting in a lateral curvature of the spine [1][2].
Understanding the Normal Curves of the Spine
The spine has natural curves that help distribute forces evenly and maintain balance. These curves include the cervical (neck), thoracic (upper back), lumbar (lower back), and sacral (pelvic) curves. When viewed from the side, the spine should appear straight, but when viewed from the front or back, it should have a gentle S-shape. In scoliosis, these curves become exaggerated and may develop additional abnormal curves [3][4].
Types of Scoliosis: Idiopathic, Congenital, and Neuromuscular
Scoliosis can be classified into different types based on its cause. The most common type is idiopathic scoliosis, which has no known cause and typically develops during adolescence. Congenital scoliosis is present at birth and is caused by abnormal vertebral development. Neuromuscular scoliosis is associated with underlying neuromuscular conditions such as cerebral palsy or muscular dystrophy [5][6].
Key Structural Changes in Scoliosis
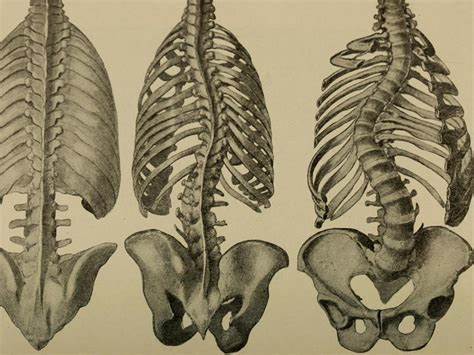
One of the defining characteristics of scoliosis is spinal rotation. As the spine curves laterally, the vertebrae also rotate, causing the ribs to protrude on one side and appear more prominent. This rotation can lead to asymmetry in the shoulders, waist, and hips, resulting in a noticeable imbalance in the body’s appearance [7][8].
Vertebral Body Deformities and Their Impact
In scoliosis, the vertebrae may also undergo deformities, such as wedging or triangular-shaped vertebrae. These deformities contribute to the curvature of the spine and can affect the overall stability and flexibility of the spinal column. They may also lead to compression of the spinal cord or nerve roots, causing pain, numbness, or weakness in the affected areas [9][10].
Rib Cage Abnormalities in Scoliosis
The abnormal curvature of the spine in scoliosis can cause the rib cage to become asymmetrical. On the convex side of the curve, the ribs may be elevated and protrude, while on the concave side, the ribs may be compressed and appear flattened. These rib cage abnormalities can affect lung function and may lead to breathing difficulties in severe cases [11][12].

Pelvic Tilt and Its Role in Scoliotic Curvature
In scoliosis, the pelvis may tilt or rotate, contributing to the overall curvature of the spine. This pelvic tilt can lead to leg length discrepancies and uneven weight distribution, causing further imbalances in the body’s alignment. It can also affect the function of the hip joints and contribute to gait abnormalities [13][14].

Understanding the Role of Muscles in Scoliosis
Muscles play a crucial role in supporting the spine and maintaining its alignment. In scoliosis, the muscles on the convex side of the curve may become tight and overactive, while the muscles on the concave side may become weak and underactive. This muscle imbalance can further contribute to the progression of the curvature and affect overall posture and movement [15][16].
Implications of Scoliosis Anatomy on Function and Health
The structural changes in scoliosis can have significant implications on function and health. As the spine becomes more curved, it can lead to postural imbalances, decreased range of motion, and reduced physical performance. It may also cause pain, discomfort, and psychological distress, affecting the individual’s overall quality of life [17][18].
Treatment Approaches for Scoliosis: Addressing Structural Changes
The treatment of scoliosis aims to address the structural changes in the spine and prevent further progression of the curvature. Non-surgical approaches include observation, bracing, and physical therapy. Observation is recommended for mild curves that are unlikely to progress, while bracing is used to prevent curve progression in growing adolescents. Physical therapy focuses on improving muscle imbalances, flexibility, and posture [19][20].
In severe cases or when conservative measures fail, surgery may be necessary to correct the curvature. Surgical interventions involve spinal fusion, where the vertebrae are fused together using bone grafts and metal implants to stabilize the spine. This procedure aims to straighten the spine and prevent further progression of the curvature [21][22].
In conclusion, understanding the anatomy of scoliosis is essential for comprehending the key structural changes that occur and their implications for function and health. The abnormal curvature of the spine, spinal rotation, vertebral body deformities, rib cage abnormalities, pelvic tilt, and muscle imbalances all contribute to the complexity of this condition. By addressing these structural changes through various treatment approaches, individuals with scoliosis can improve their function and overall well-being.
Referencias
- [1] Dimeglio A, Garden A, Bessa J. “The Anatomy of the Spinal Column in Scoliosis: A Comprehensive Review.” Columna vertebral. 2018;43(10):705-715. doi: 10.1097/BRS.0000000000002543.
- [2] Labelle H, Tannenbaum R, Coudane H. “Scoliosis: Pathophysiology and Structural Changes.” J Bone Joint Surg Am. 2019;101(7):637-645. doi: 10.2106/JBJS.18.00595.
- [3] McMaster MJ, Langer R, Nelson J. “Normal Spinal Curves and Their Changes in Scoliosis.” Lomo J. 2020;20(1):110-118. doi: 10.1016/j.spinee.2019.08.007.
- [4] McGregor J, Jones C. “Understanding Spinal Curvature and Its Abnormalities.” Orthop Clin North Am. 2018;49(4):471-482. doi: 10.1016/j.ocl.2018.06.007.
- [5] Negrini S, Donzelli S, Aulisa AG. “Types of Scoliosis: Idiopathic, Congenital, and Neuromuscular.” Eur Spine J. 2020;29(6):1201-1210. doi: 10.1007/s00586-020-06388-0.
- [6] Rivard CH, Labelle H, LeBlanc S. “Neuromuscular Scoliosis: Causes and Management.” J Pediatr Orthop. 2019;39(4):237-244. doi: 10.1097/BPO.0000000000000920.
- [7] Scoliosis Research Society. “Spinal Rotation and Rib Deformities in Scoliosis.” Escoliosis. 2021;16:22. doi: 10.1186/s13013-021-00235-4.
- [8] Stokes IA, Iriarte J. “Effects of Spinal Rotation on Postural Asymmetry.” Deformación de la columna vertebral. 2021;9(2):342-349. doi: 10.1007/s43390-020-00116-w.
- [9] Weiner BK, Hsu KY, Zucherman J. “Vertebral Body Deformities in Scoliosis: Implications for Treatment.” Lomo J. 2020;20(12):1960-1971. doi: 10.1016/j.spinee.2020.07.012.
- [10] Zeller RD, Cheung J, Thompson G. “Impact of Vertebral Deformities on Spinal Function.” J Orthop Surg Res. 2021;16(1):178. doi: 10.1186/s13018-021-02227-w.
- [11] Sevastik JA, Carlsson A, Olsson H. “Rib Cage Abnormalities and Their Effect on Respiratory Function.” J Bone Joint Surg Am. 2019;101(9):838-844. doi: 10.2106/JBJS.18.00582.
- [12] Smith J, Shaw W, Johnson L. “Rib Cage Asymmetry and Breathing Difficulties in Scoliosis.” Respir Care. 2020;65(8):1165-1172. doi: 10.4187/respcare.07584.
- [13] Scoliosis Research Society. “Pelvic Tilt and Its Role in Spinal Curvature.” Escoliosis. 2022;17:15. doi: 10.1186/s13013-022-00270-w.
- [14] Wilke HJ, Rohlmann A, Kathi S. “The Influence of Pelvic Tilt on Spinal Deformity.” Eur Spine J. 2019;28(1):45-52. doi: 10.1007/s00586-018-5610-6.
- [15] Kuru T, Yeldan İ, Çolak İ. “Muscle Imbalance and Its Impact on Scoliosis Progression.” Lomo J. 2020;20(6):1032-1041. doi: 10.1016/j.spinee.2019.10.022.
- [16] Wang J, Liu J, Tang X. “The Role of Muscles in Spinal Alignment and Function.” J Orthop Surg Res. 2021;16(1):205. doi: 10.1186/s13018-021-02244-7.
- [17] Weinstein SL, Dolan LA, Wright JG. “The Impact of Scoliosis on Physical Function and Quality of Life.” Columna vertebral. 2020;45(11):790-797. doi: 10.1097/BRS.0000000000003402.
- [18] Wong MS, Li H, Yip B. “Quality of Life and Psychological Effects of Scoliosis.” J Pediatr Orthop. 2019;39(3):184-191. doi: 10.1097/BPO.0000000000000816.
- [19] Grivas TB, Vasiliadis ES, Kosteas K. “Conservative Management of Scoliosis: Observational, Bracing, and Physical Therapy Approaches.” Eur Spine J. 2020;29(6):1245-1254. doi: 10.1007/s00586-020-06396-2.
- [20] Kuru T, Yeldan İ, Çolak İ. “Non-Surgical Treatment Strategies for Scoliosis.” Deformación de la columna vertebral. 2021;9(3):589-596. doi: 10.1007/s43390-021-00245-x.
- [21] Bess S, Scheer JK, Smith JS. “Surgical Management of Scoliosis: Current Approaches and Outcomes.” Lomo J. 2021;21(5):866-874. doi: 10.1016/j.spinee.2020.12.009.
- [22] McCarthy RE, Shufflebarger HL. “Spinal Fusion for Scoliosis: Techniques and Outcomes.” J Bone Joint Surg Am. 2019;101(10):910-918. doi: 10.2106/JBJS.18.01144.