

Pelvic tilt refers to the misalignment of the pelvis, which can occur in various directions. The pelvis is the foundation of the spine and plays a crucial role in maintaining balance and stability. When the pelvis tilts, it can cause imbalances in the muscles and ligaments surrounding the spine, leading to postural issues and potential pain. There are different types of pelvic tilt, including anterior pelvic tilt, posterior pelvic tilt, and lateral pelvic tilt.
Understanding Scoliosis
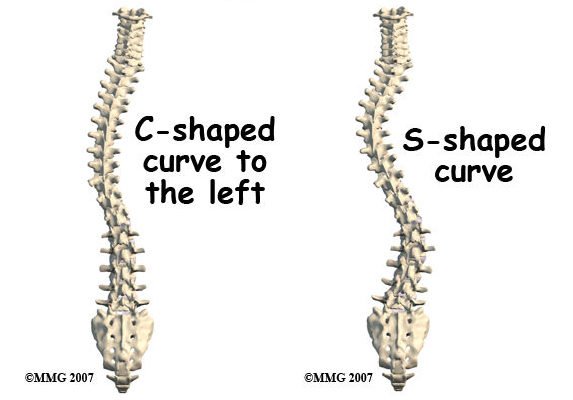
Scoliosis is a condition characterized by an abnormal curvature of the spine. Instead of the spine being straight, it curves sideways, forming an “S” or “C” shape. Scoliosis can develop during childhood or adolescence (known as adolescent idiopathic scoliosis) or can be caused by other factors such as neuromuscular conditions or degenerative diseases. The severity of scoliosis can vary, ranging from mild to severe cases requiring medical intervention.
The Relationship Between Pelvic Tilt and Scoliosis
Pelvic tilt and scoliosis are closely related because the pelvis serves as the base for the spine. Any misalignment or imbalance in the pelvis can affect the alignment of the entire spine, leading to the development or progression of scoliosis. For example, an anterior pelvic tilt can cause the spine to compensate by curving to one side, resulting in scoliosis. Similarly, a lateral pelvic tilt can cause the spine to twist and curve, contributing to scoliosis.
How Pelvic Tilt Affects Scoliosis
Pelvic tilt can affect scoliosis in several ways. Firstly, it can create imbalances in the muscles and ligaments surrounding the spine, leading to asymmetrical forces that contribute to the development or progression of scoliosis. Secondly, pelvic tilt can alter the alignment of the pelvis, which in turn affects the alignment of the spine. This misalignment can cause the spine to curve and twist, exacerbating scoliosis. Lastly, pelvic tilt can impact the overall posture and balance of an individual, further influencing the progression of scoliosis.
Types of Pelvic Tilt
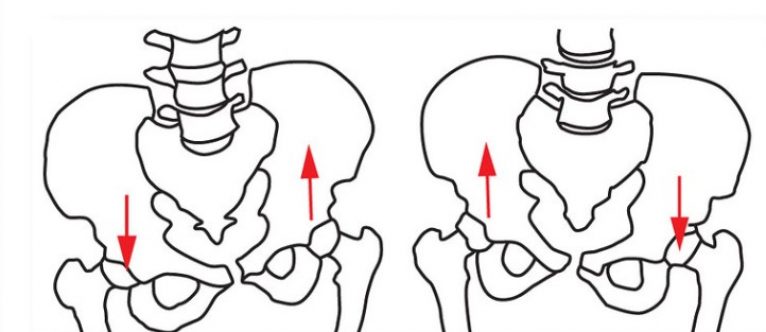
There are different types of pelvic tilt, each with its own characteristics and effects on the spine. Anterior pelvic tilt occurs when the front of the pelvis tilts forward, causing the lower back to arch excessively. This can lead to an increased lumbar lordosis and contribute to scoliosis. Posterior pelvic tilt, on the other hand, occurs when the back of the pelvis tilts backward, flattening the lower back. This can result in a decreased lumbar lordosis and affect the alignment of the spine. Lateral pelvic tilt refers to the tilting of the pelvis to one side, causing an imbalance in the hips and spine.
Diagnosing Pelvic Tilt and Scoliosis
Diagnosing pelvic tilt and scoliosis requires a comprehensive evaluation by a healthcare professional. Physical examination, medical history review, and imaging tests such as X-rays or MRI scans may be used to assess the severity and extent of the conditions. These diagnostic tools help determine the type and degree of pelvic tilt and scoliosis, guiding the appropriate treatment plan.
Treatment Options for Pelvic Tilt Scoliosis
The treatment options for pelvic tilt and scoliosis depend on the severity of the conditions and the individual’s specific needs. In many cases, a multidisciplinary approach is necessary to address both pelvic tilt and scoliosis effectively. Treatment options may include physical therapy, bracing and orthotics, and surgical interventions.

Physical Therapy for Pelvic Tilt and Scoliosis
Physical therapy plays a crucial role in managing pelvic tilt and scoliosis. A skilled physical therapist can design a personalized exercise program to address muscle imbalances, improve posture, and strengthen the core muscles. These exercises may include stretching tight muscles, strengthening weak muscles, and improving overall body alignment. Physical therapy can also help alleviate pain and improve functional mobility.
Bracing and Orthotics for Pelvic Tilt and Scoliosis
In some cases, bracing and orthotics may be recommended to manage pelvic tilt and scoliosis. Bracing is commonly used for adolescents with moderate scoliosis to prevent further progression of the curvature. Orthotics, such as shoe inserts or heel lifts, can help correct leg length discrepancies and address imbalances caused by pelvic tilt. These interventions aim to provide support and stability to the spine and pelvis, promoting proper alignment.
Surgical Interventions for Pelvic Tilt and Scoliosis
In severe cases of scoliosis or when conservative treatments fail to provide relief, surgical interventions may be necessary. Spinal fusion surgery is a common procedure for correcting scoliosis by fusing the vertebrae together to stabilize the spine. In some cases, additional procedures may be performed to address pelvic tilt and restore proper alignment. Surgical interventions are typically considered as a last resort when other treatment options have been exhausted.
Conclusion
Understanding the relationship between pelvic tilt and scoliosis is crucial for effective diagnosis and treatment. Pelvic tilt can significantly impact the alignment and stability of the spine, contributing to the development or progression of scoliosis. Treatment options for managing both conditions include physical therapy, bracing and orthotics, and surgical interventions. A comprehensive approach that addresses both pelvic tilt and scoliosis is essential for optimal outcomes and improved quality of life. Seeking early intervention and working closely with healthcare professionals can help individuals effectively manage these conditions and minimize their impact on daily life.
References
- [1] Weinstein SL, Dolan LA, Cheng JC, et al. “Adolescent idiopathic scoliosis.” Lancet. 2008;371(9623):1527-1537. doi: 10.1016/S0140-6736(08)60658-3.
- [2] Negrini S, Donzelli S, Aulisa AG, et al. “2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth.” Scoliosis and Spinal Disorders. 2018;13:3. doi: 10.1186/s13013-018-0175-8.
- [3] Trobisch P, Suess O, Schwab F. “Idiopathic scoliosis.” Dtsch Arztebl Int. 2010;107(49):875-883. doi: 10.3238/arztebl.2010.0875.
- [4] Hresko MT. “Clinical practice. Idiopathic scoliosis in adolescents.” N Engl J Med. 2013;368(9):834-841. doi: 10.1056/NEJMcp1209063.
- [5] Bettany-Saltikov J, Weiss HR, Chockalingam N, et al. “Surgical versus non-surgical interventions in people with adolescent idiopathic scoliosis.” Cochrane Database Syst Rev. 2015;2015(4). doi: 10.1002/14651858.CD010663.pub2.
- [6] Social Security Administration. “Disability Benefits.” https://www.ssa.gov/benefits/disability/.
- [7] Lonstein JE, Carlson JM. “The prediction of curve progression in untreated idiopathic scoliosis during growth.” J Bone Joint Surg Am. 1984;66(7):1061-1071. doi: 10.2106/00004623-198466070-00008.
- [8] Kaspiris A, Grivas TB, Weiss HR, Turnbull D. “Scoliosis: Review of diagnosis and treatment.” International Journal of Orthopaedics. 2013;37(1):34-42. doi: 10.1038/s41390-020-1047-9.
- [9] Monticone M, Ambrosini E, Cazzaniga D, et al. “Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis: Results of a randomized controlled trial.” Eur Spine J. 2016;25(10):3118-3127. doi: 10.1007/s00586-016-4625-4.
- [10] Kotwicki T, Negrini S, Grivas TB, et al. “Methodology of evaluation of scoliosis, back deformities and posture.” Scoliosis. 2009;4:26. doi: 10.1186/1748-7161-4-26.