

Scoliosis is a complex spinal deformity that affects millions of people worldwide. Traditionally, the mainstay of treatment for scoliosis has been spinal fusion surgery. However, this invasive procedure comes with its limitations and challenges. In recent years, there has been a growing interest in non-fusion techniques for scoliosis correction, with tethering scoliosis emerging as an innovative and promising approach. This article aims to provide a comprehensive overview of tethering scoliosis, including its definition, mechanism, benefits, types of techniques, case studies, potential risks, and future directions.
Understanding Scoliosis and its Impact
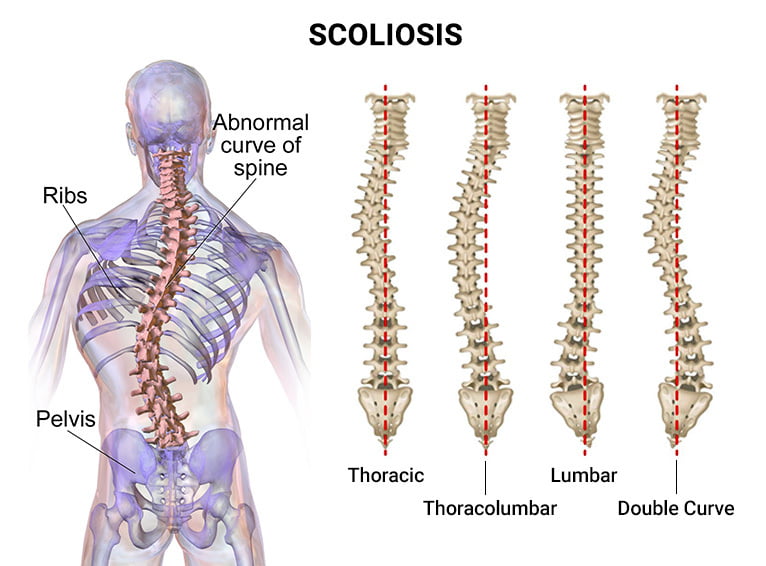
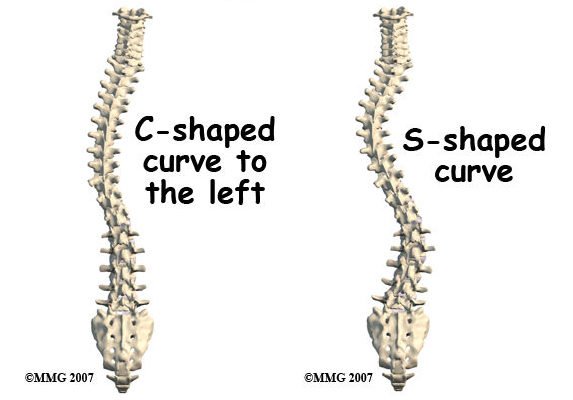
Scoliosis is a condition characterized by an abnormal curvature of the spine, often in an “S” or “C” shape. It can develop during childhood or adolescence and can have a significant impact on a person’s physical appearance, function, and overall quality of life. The severity of scoliosis can vary, with some cases requiring intervention to prevent further progression and potential complications such as respiratory problems and chronic pain.
Traditional Fusion Techniques for Scoliosis Correction
For many years, spinal fusion surgery has been the gold standard for scoliosis correction. This procedure involves fusing together two or more vertebrae using bone grafts and metal implants to straighten and stabilize the spine. While fusion techniques have been successful in reducing the curvature of the spine, they come with several limitations and challenges.
Limitations and Challenges of Fusion Techniques
One of the main limitations of fusion techniques is the loss of spinal flexibility. The fused segments of the spine become rigid, limiting the range of motion and potentially leading to adjacent segment disease. Additionally, fusion surgery requires a long recovery period, often involving the use of braces and physical therapy. Furthermore, fusion techniques may not be suitable for all patients, especially those with flexible curves or young children who are still growing.
Introduction to Non-Fusion Techniques for Scoliosis Correction
Non-fusion techniques for scoliosis correction aim to address the limitations of fusion surgery by preserving spinal flexibility and allowing for continued growth. Tethering scoliosis is one such non-fusion technique that has gained attention in recent years.

Tethering Scoliosis: Definition and Mechanism
Tethering scoliosis involves the use of flexible materials, such as screws, cables, or straps, to correct the curvature of the spine. These materials are attached to the vertebrae and act as a “tether,” guiding the growth of the spine in a more desirable direction. The tethering technique allows for continued growth and flexibility while still providing correction and stabilization.
Benefits and Advantages of Tethering Scoliosis
One of the key benefits of tethering scoliosis is the preservation of spinal flexibility. Unlike fusion techniques, which restrict movement, tethering allows for continued growth and natural motion of the spine. This can lead to improved long-term outcomes and a reduced risk of adjacent segment disease. Additionally, tethering scoliosis can be performed on younger patients who are still growing, providing an alternative to fusion surgery.
Types of Tethering Scoliosis Techniques
There are several types of tethering scoliosis techniques, each with its own unique approach and materials used. Some common techniques include vertebral body tethering (VBT), anterior vertebral body tethering (AVBT), and posterior vertebral body tethering (PVBT). VBT involves placing screws into the vertebral bodies and connecting them with a flexible cord, while AVBT and PVBT involve placing screws and attaching them to the front or back of the vertebrae, respectively.
Case Studies: Successful Tethering Scoliosis Corrections
Numerous case studies have demonstrated the effectiveness of tethering scoliosis in correcting spinal deformities. For example, a study published in the Journal of Pediatric Orthopaedics reported successful correction of scoliosis in a group of adolescent patients using VBT. The study showed significant improvements in spinal curvature and patient satisfaction, with minimal complications.
Potential Risks and Complications of Tethering Scoliosis
While tethering scoliosis offers promising results, it is not without risks and potential complications. Some potential risks include implant failure, loss of correction, and the need for revision surgery. Additionally, there is limited long-term data on the outcomes of tethering scoliosis, making it important for patients and surgeons to carefully consider the potential risks and benefits before choosing this technique.
Future Directions and Innovations in Tethering Scoliosis
As with any evolving field, there are ongoing research and innovations in tethering scoliosis. Researchers are exploring new materials and techniques to improve the outcomes and safety of tethering procedures. For example, biodegradable implants are being investigated to reduce the risk of long-term complications. Additionally, advancements in imaging technology and surgical techniques are allowing for more precise and personalized tethering procedures.
Conclusion: The Promising Future of Tethering Scoliosis Correction
Tethering scoliosis represents an innovative and promising approach to scoliosis correction. By preserving spinal flexibility and allowing for continued growth, tethering techniques offer potential advantages over traditional fusion surgery. While there are risks and challenges associated with tethering scoliosis, ongoing research and advancements in the field are likely to further improve outcomes and expand the applicability of this technique. As more data and long-term studies become available, tethering scoliosis may become a mainstream option for scoliosis correction, providing patients with a less invasive and more flexible treatment option.
Références
- Weinstein SL, Dolan LA, Cheng JC, et al. "Adolescent idiopathic scoliosis". Lancet. 2008;371(9623):1527-1537. doi : 10.1016/S0140-6736(08)60658-3.
- Negrini S, Donzelli S, Aulisa AG, et al. "2016 SOSORT guidelines : Traitement orthopédique et de rééducation de la scoliose idiopathique pendant la croissance." Scoliose et troubles de la colonne vertébrale. 2018;13:3. doi : 10.1186/s13013-018-0175-8.
- Trobisch P, Suess O, Schwab F. "Scoliose idiopathique". Dtsch Arztebl Int. 2010;107(49):875-883. doi : 10.3238/arztebl.2010.0875.
- Hresko MT. "Pratique clinique. Scoliose idiopathique chez les adolescents". N Engl J Med. 2013;368(9):834-841. doi : 10.1056/NEJMcp1209063.
- Bettany-Saltikov J, Weiss HR, Chockalingam N, et al. "Surgical versus non-surgical interventions in people with adolescent idiopathic scoliosis". Cochrane Database Syst Rev. 2015;2015(4). doi : 10.1002/14651858.CD010663.pub2.
- Administration de la sécurité sociale. "Prestations d'invalidité". Administration de la sécurité sociale. Disponible à l'adresse suivante : https://www.ssa.gov/benefits/disability/.
- Lonstein JE, Carlson JM. "The prediction of curve progression in untreated idiopathic scoliosis during growth" (La prédiction de la progression de la courbe dans la scoliose idiopathique non traitée pendant la croissance). J Bone Joint Surg Am. 1984;66(7):1061-1071. doi : 10.2106/00004623-198466070-00008.
- Kaspiris A, Grivas TB, Weiss HR, Turnbull D. "Scoliosis : Examen du diagnostic et du traitement". Journal international d'orthopédie. 2013;37(1):34-42. doi : 10.1038/s41390-020-1047-9.
- Monticone M, Ambrosini E, Cazzaniga D, et al. "Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis : Results of a randomized controlled trial". Eur Spine J. 2016;25(10):3118-3127. doi : 10.1007/s00586-016-4625-4.
- Kotwicki T, Negrini S, Grivas TB, et al. "Methodology of evaluation of scoliosis, back deformities and posture". Scoliose. 2009;4:26. doi : 10.1186/1748-7161-4-26.