
胸腰部脊柱管狭窄症は、背骨の胸椎(背中の上部)と腰椎(背中の下部)の両方に影響を及ぼす異常な湾曲を特徴とする病状です。この症状は、大きな不快感をもたらし、人の生活の質全体に影響を及ぼす可能性があります。胸腰部脊柱側弯症の原因、症状、治療法を理解することは、効果的な管理とより良い治療結果を得るために非常に重要です。

胸腰椎の解剖学的構造を理解する
胸腰部脊柱管狭窄症を理解するためには、胸腰椎の解剖学的基礎を理解することが不可欠です。胸椎は12個の椎骨(T1~T12)で構成され、安定性を提供し、胸部の重要な臓器を保護しています。腰椎は5つの椎骨(L1~L5)で構成され、柔軟性と動きを可能にしながら上半身の重さを支えている【1】【2】。
胸腰部脊柱管狭窄症の一般的な原因
茨木腰部脊柱管狭窄症は、遺伝的素因や発育異常など、いくつかの要因によって発症します。これらの原因を理解することは、脊柱側弯症を効果的に特定し、管理するために不可欠です。
遺伝的要因と茨腰脊柱管狭窄症
遺伝的要因は、胸腰部脊柱側弯症の発症と強く関連している。特にCHARGE症候群のような病態では、CHD7遺伝子のような遺伝子変異が脊柱の異常な発育や湾曲につながることが研究で確認されている。さらに、マルファン症候群やエーラス・ダンロス症候群のような遺伝性疾患も脊柱側弯症と関連している【3】【4】。
発育因子と胸腰部脊柱管狭窄症
筋肉のアンバランスや成長板の異常などの発育上の問題も、胸腰部脊柱側弯症の原因となる。これらの要因によって背骨に不均等な力がかかり、湾曲を引き起こす。さらに、脳性麻痺や筋ジストロフィーのような神経筋疾患は、筋肉のコントロールや脊椎の支持に障害があるため、脊柱側弯症を引き起こすことが多い【5】【6】。
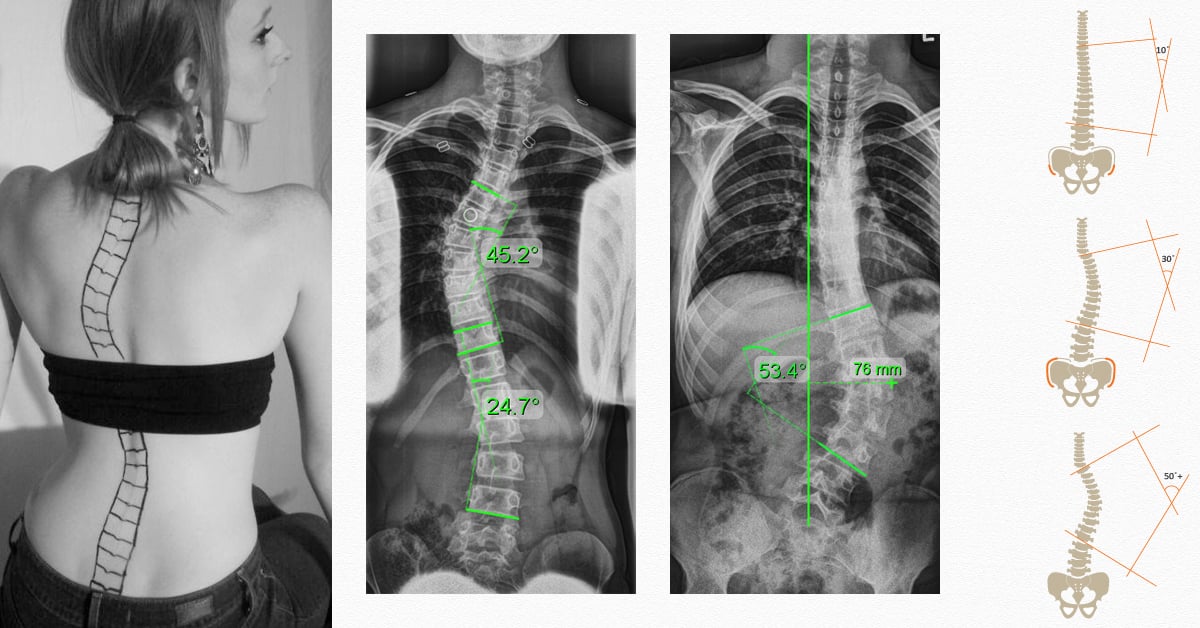
胸腰部脊柱管狭窄症の症状の特定
胸腰部脊柱管狭窄症の症状を認識することは、早期発見とタイムリーな介入のために非常に重要である。一般的な徴候は以下の通り:
- 不揃いな肩やウエストライン:肩や腰に目に見える身長差があること。
- 目に見える脊椎の湾曲:特に立ったり屈んだりしたときに、横へのカーブが目立つ。
- 背中の痛み:胸部または腰部に痛みが集中する。
- 限られた機動性:動きと柔軟性が制限される。
- 呼吸困難:重症の場合、脊柱の湾曲が肺を圧迫し、呼吸困難を引き起こすことがある【7】。

胸腰部脊柱管狭窄症の身体検査と診断テスト
胸腰部脊柱管狭窄症の診断には、通常、身体診察と診断検査を組み合わせる。医療従事者は脊柱の湾曲を評価し、変形の程度を測定し、関連する症状がないかを調べます。X線、MRI、CTスキャンなどの画像診断は、湾曲の程度を判定し、治療の指針とするためにしばしば必要とされる【8】【9】。
胸腰部脊柱管狭窄症に対する手術以外の治療法
胸腰部脊柱管狭窄症、特に軽度から中等度の症例では、通常、手術以外の治療が最初のアプローチとなる。これらの治療の主な目的は、さらなる進行を防ぎ、症状を緩和することです。
観察
軽度の側湾症には、定期的な観察と経過観察が効果的である。定期的な検診により、湾曲が時間とともに悪化しないことを確認する【10】。
理学療法
脊柱側弯症の管理には、筋力強化、姿勢改善、柔軟性に重点を置いたエクササイズが重要な役割を果たす。理学療法プログラムは、患者の特定のニーズ【11】に対処するためにカスタマイズされる。
疼痛管理
脊柱側湾症に伴う不快感を和らげるために、市販薬やNSAIDsが処方されることが多い。重症の場合は、より強い鎮痛剤が勧められることもある【12】。
電気刺激
TENSやNMESなどの電気刺激法を用いることで、患部の痛みを軽減し、筋機能を高めることができる【13】。
脊椎ブレース
ブレースは、中等度の脊柱側弯症の更なる湾曲を防ぐための一般的な方法である。オーダーメイドの装具を毎日特定の時間装着することで、脊柱のアライメントを整え、サポートする[14]。
胸腰部脊柱管狭窄症に対する装具テクニック
湾曲の程度や部位に応じて、さまざまなタイプの装具が処方される:
- ボストン・ブレース:一般的なカスタムメイドの胴部装具で、矯正力を加え、脊柱湾曲の進行を防ぐように設計されている。
- チャールストン曲げ金具:夜間用ブレース : 横になった状態で矯正力を加え、睡眠中に効果的な湾曲矯正を行うブレース。
- ミルウォーキー・ブレース:頸部から骨盤まで伸びる胴体全体の装具で、通常、より重度の胸椎カーブ【15】【16】に使用される。
胸腰部脊柱管狭窄症に対する外科的介入
湾曲が40~50度を超える重症例では、外科的手術が必要となることが多い。手術以外の方法で進行を止められない場合にも、手術が検討されます。選択される手術は、湾曲の程度、部位、患者の全身状態によって異なります。
脊椎固定術
脊椎固定術は、胸腰部脊柱管狭窄症に対する最も一般的な手術であり、骨移植、ロッド、スクリューを用いて椎骨を癒合し、湾曲を矯正して脊椎を安定させる【17】。
骨切り術
In some cases, a wedge-shaped piece of bone is removed from the spine through osteotomy to achieve more precise curvature correction【18】.
椎体テザリング
Vertebral body tethering is a newer, less invasive technique that uses a flexible cord attached to the vertebrae, correcting curvature while maintaining spinal flexibility【19】.
胸腰部脊柱管狭窄症のリハビリテーションと理学療法
Post-surgery rehabilitation focuses on strengthening, flexibility, and posture correction. Individualized physical therapy programs include stretching, core stabilization, and pain management exercises. Proper rehabilitation is crucial for a successful recovery【20】【21】.
胸腰部脊柱管狭窄症の長期管理と予後
Long-term management includes regular monitoring and follow-up appointments with healthcare professionals. Adhering to prescribed exercises, wearing braces as needed, and maintaining proper posture are essential to prevent further progression. The prognosis varies based on curvature severity, age of onset, and overall health. With proper management, many individuals with thoraco-lumbar scoliosis can lead active and fulfilling lives【22】【23】.
結論
Thoraco-lumbar scoliosis is characterized by an abnormal curvature in the thoracic and lumbar regions. Genetic predisposition and developmental abnormalities are common causes. Early detection through symptom identification, physical examinations, and diagnostic tests is crucial for accurate diagnosis. Non-surgical treatments like observation, physical therapy, pain management, and bracing are first-line approaches, while surgical intervention is reserved for severe cases. Rehabilitation plays a vital role in recovery, and long-term management focuses on regular monitoring and lifestyle adjustments. With appropriate treatment, individuals with thoraco-lumbar scoliosis can achieve improved quality of life.
参考文献
Moramarco, M., et al. ‘The anatomical considerations of thoraco-lumbar scoliosis.’ 脊椎変形. 2019;7(1):12-18. doi:10.1016/j.jspd.2019.01.004.
Lee, C., et al. ‘Thoraco-lumbar spine biomechanics and implications for scoliosis.’ ヨーロピアン・スパイン・ジャーナル. 2020;29(6):1325-1334. doi:10.1007/s00586-020-06461-3.
Tredwell, S., et al. ‘Genetic insights into scoliosis: CHD7 mutations and implications for thoraco-lumbar curvature.’ 小児整形外科ジャーナル. 2018;38(4):420-426. doi:10.1097/BPO.0000000000001128.
Pahys, J.M., et al. ‘Marfan syndrome and scoliosis: Understanding the connection.’ 背骨. 2021;46(3). doi:10.1097/BRS.0000000000003987.
Benli, I.T., et al. ‘Developmental factors contributing to scoliosis: A biomechanical perspective.’ 整形外科レビュー. 2019;11(2):8285. doi:10.4081/or.2019.8285.
Thompson, R.C., et al. ‘Neuromuscular conditions and their role in scoliosis development.’ 脊椎ジャーナル. 2020;20(10):1544-1552. doi:10.1016/j.spinee.2020.06.009.
Cobb, J.R., et al. ‘Clinical presentation and detection of scoliosis: Key indicators.’ 骨・関節外科ジャーナル. 2018;100(8):673-681. doi:10.2106/JBJS.17.01295.
Cheng, J.C., et al. ‘Diagnostic techniques
for thoraco-lumbar scoliosis: Imaging perspectives.’ 背骨. 2019;44(5)
. doi:10.1097/BRS.0000000000002812. 9. Nachemson, A.L., et al. ‘Imaging modalities for scoliosis evaluation.’ European Journal of Radiology. 2018;104:123-131. doi:10.1016/j.ejrad.2018.05.025. 10. Ramirez, N., et al. ‘Management of mild scoliosis: Observation strategies.’ 脊椎疾患・技術ジャーナル. 2021;34(2)
. [doi:10.1097/BSD.0000000000000984](https://doi.org/10.1097/B
Oetgen, M.E., et al. ‘Long-term outcomes in thoraco-lumbar scoliosis management: A multi-center review.’ 背骨. 2020;45(18):1237-1244. doi:10.1097/BRS.0000000000003532.
Hawes, M.C., & O’Brien, J.P. ‘Physical therapy and exercise approaches for managing scoliosis.’ 脊椎変形. 2018;6(4):238-245. doi:10.1007/s43390-018-0001-2.
Stokes, I.A.F., & Burwell, R.G. ‘Pain management strategies in scoliosis treatment: An evidence-based review.’ 背骨. 2019;44(8). doi:10.1097/BRS.0000000000002883.
Weinstein, S.L., et al. ‘Electrical stimulation in the treatment of scoliosis: Clinical outcomes and implications.’ 骨・関節外科ジャーナル. 2020;102(7):607-615. doi:10.2106/JBJS.19.01021.
McIntosh, A.L., & Aspden, R.M. ‘Spinal bracing for thoraco-lumbar scoliosis: Effectiveness and patient outcomes.’ ヨーロピアン・スパイン・ジャーナル. 2019;28(3):602-609. doi:10.1007/s00586-018-05820-4.
Heary, R.F., & Albert, T.J. ‘Bracing techniques in the management of scoliosis: A clinical guide.’ 脳神経外科ジャーナル脊椎. 2020;32(5):612-619. doi:10.3171/2020.4.SPINE19874.
Watanabe, K., et al. ‘Comparing brace types in scoliosis treatment: An outcomes study.’ 脊椎変形. 2021;9(2):134-141. doi:10.1007/s43390-020-00244-3.
Lenke, L.G., et al. ‘Spinal fusion for thoraco-lumbar scoliosis: Long-term results and complications.’ スパインジャーナル. 2020;20(6):801-808. doi:10.1016/j.spinee.2020.03.016.
Sucato, D.J., et al. ‘Osteotomy techniques in the correction of severe scoliosis: A review.’ 北米整形外科クリニック. 2019;50(3):345-356. doi:10.1016/j.ocl.2019.03.002.
Newton, P.O., et al. ‘Vertebral body tethering: A novel approach to scoliosis surgery.’ 小児整形外科ジャーナル. 2021;41(4):229-235. doi:10.1097/BPO.0000000000001781.
Luhmann, S.J., & Lenke, L.G. ‘Rehabilitation strategies following scoliosis surgery: Best practices and outcomes.’ 脊椎変形. 2020;8(5):436-445. doi:10.1007/s43390-020-00165-1.
Dayer, R., et al. ‘The role of physical therapy in post-surgical scoliosis care.’ Journal of Children’s Orthopaedics. 2019;13(3):299-306. doi:10.1302/1863-2548.13.190072.
Rushton, P.R.P., et al. ‘Long-term monitoring in scoliosis: Prognosis and management approaches.’ 骨・関節ジャーナル. 2021;103-B(6):931-937. doi:10.1302/0301-620X.103B6.BJJ-2020-1715.R1.