

Scoliosis is a medical condition characterized by an abnormal curvature of the spine. It affects millions of people worldwide, with varying degrees of severity. For individuals living with scoliosis, the impact on their daily lives can be significant, leading to functional limitations and impairments that may affect their ability to perform activities of daily living (ADLs) and work-related tasks. In order to provide appropriate support and resources, it is crucial to assess and determine the disability levels associated with scoliosis. This article will delve into the various aspects of assessing and determining scoliosis-related disability levels, including understanding scoliosis, types and causes of scoliosis, medical evaluation and diagnosis, imaging techniques for scoliosis assessment, functional limitations and impairments, evaluating ADLs, assessing work-related limitations, the social and emotional impact of scoliosis, disability rating systems, and determining scoliosis-related disability levels.
Compreender a escoliose
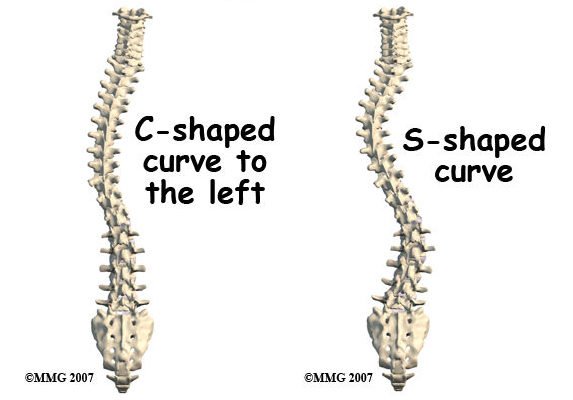
Scoliosis is a condition that causes an abnormal sideways curvature of the spine. It can occur at any age, but it is most commonly diagnosed during adolescence. The curvature can be either “C” shaped or “S” shaped, and it can range from mild to severe. The exact cause of scoliosis is often unknown, but it can be influenced by factors such as genetics, muscle imbalances, and neuromuscular conditions. It is important to note that scoliosis is not a result of poor posture or carrying heavy backpacks, as these are common misconceptions.
Tipos e causas de escoliose
There are several types of scoliosis, including idiopathic scoliosis, congenital scoliosis, neuromuscular scoliosis, and degenerative scoliosis. Idiopathic scoliosis is the most common type and occurs without a known cause. Congenital scoliosis is present at birth and is caused by abnormal spinal development. Neuromuscular scoliosis is associated with conditions such as cerebral palsy or muscular dystrophy, while degenerative scoliosis is a result of age-related changes in the spine.
Assessing Scoliosis-Related Disability
Assessing scoliosis-related disability involves a comprehensive evaluation of the individual’s medical history, physical examination, imaging techniques, functional limitations, and impact on activities of daily living (ADLs) and work-related tasks. This assessment is crucial in determining the level of disability and the appropriate support and resources needed for the individual.
Medical Evaluation and Diagnosis
A medical evaluation is the first step in assessing scoliosis-related disability. It involves a thorough review of the individual’s medical history, including any previous diagnoses, treatments, and surgeries. The healthcare provider will also conduct a physical examination to assess the curvature of the spine, range of motion, and any associated symptoms such as pain or neurological deficits. During the examination, the healthcare provider may use a scoliometer, a device that measures the degree of spinal curvature.
Imaging Techniques for Scoliosis Assessment
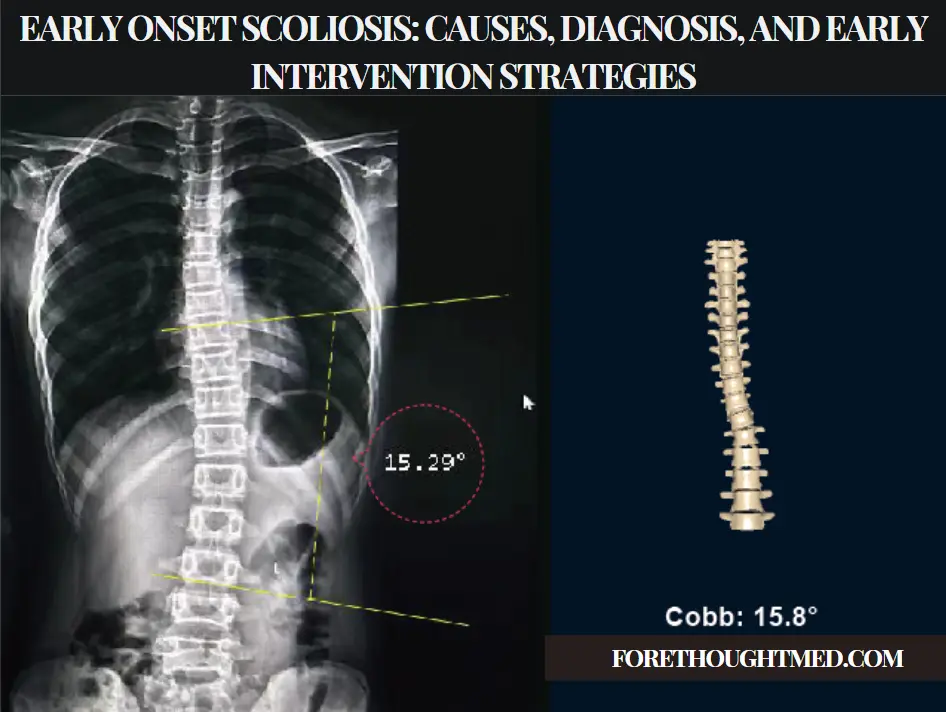
Imaging techniques play a crucial role in assessing scoliosis. X-rays are commonly used to evaluate the severity and progression of the curvature. X-rays provide detailed images of the spine, allowing healthcare providers to measure the degree of curvature and identify any structural abnormalities. Other imaging techniques, such as magnetic resonance imaging (MRI) or computed tomography (CT) scans, may be used in specific cases to further evaluate the spine and surrounding structures.
Functional Limitations and Impairments
Scoliosis can lead to functional limitations and impairments that affect an individual’s ability to perform daily activities. These limitations can include difficulties with mobility, balance, and coordination. The severity of these limitations varies depending on the degree of spinal curvature and any associated symptoms. For example, individuals with severe scoliosis may experience difficulty walking or standing for long periods of time, while those with milder forms may have minimal functional limitations.
Evaluating Activities of Daily Living (ADLs)
Assessing the impact of scoliosis on activities of daily living (ADLs) is crucial in determining disability levels. ADLs refer to the basic tasks necessary for self-care, such as bathing, dressing, eating, and toileting. Scoliosis can affect an individual’s ability to perform these tasks independently, especially if the curvature of the spine restricts movement or causes pain. Healthcare providers may use standardized assessment tools to evaluate the individual’s ability to perform ADLs and identify any modifications or assistive devices needed.
Assessing Work-Related Limitations
Scoliosis can also impact an individual’s ability to perform work-related tasks. Depending on the severity of the curvature and associated symptoms, individuals with scoliosis may experience limitations in physical activities, such as lifting, carrying, or prolonged sitting or standing. These limitations can affect various occupations, from manual labor to desk jobs. Healthcare providers may assess the individual’s work-related limitations through functional capacity evaluations or job-specific assessments to determine the level of disability and the need for workplace accommodations.
Social and Emotional Impact of Scoliosis
In addition to the physical limitations, scoliosis can have a significant social and emotional impact on individuals. The visible curvature of the spine may lead to self-consciousness, body image issues, and decreased self-esteem. It can also affect social interactions, as individuals may feel stigmatized or excluded due to their condition. It is important to consider the social and emotional aspects of scoliosis when assessing disability levels, as they can greatly impact an individual’s overall well-being and quality of life.
Disability Rating Systems
Disability rating systems are used to assess and determine the level of disability associated with various medical conditions, including scoliosis. These systems provide a standardized framework for evaluating the impact of the condition on an individual’s functional abilities and limitations. Examples of disability rating systems include the International Classification of Functioning, Disability, and Health (ICF), the American Medical Association’s Guides to the Evaluation of Permanent Impairment (AMA Guides), and the Social Security Administration’s Listing of Impairments.
Determining Scoliosis-Related Disability Levels
Determining scoliosis-related disability levels involves a comprehensive evaluation of the individual’s medical history, physical examination, imaging results, functional limitations, impact on ADLs and work-related tasks, and the social and emotional impact of the condition. Healthcare providers, including orthopedic surgeons, physical therapists, and occupational therapists, play a crucial role in this process. They use a combination of clinical judgment, standardized assessment tools, and disability rating systems to determine the level of disability and recommend appropriate support and resources for the individual.
In conclusion, assessing and determining scoliosis-related disability levels is a complex process that requires a comprehensive evaluation of various factors. Understanding scoliosis, its types and causes, medical evaluation and diagnosis, imaging techniques, functional limitations, impact on ADLs and work-related tasks, social and emotional impact, disability rating systems, and the overall determination of disability levels are all crucial in providing appropriate support and resources for individuals living with scoliosis. By considering these factors, healthcare providers can ensure that individuals with scoliosis receive the necessary assistance to enhance their quality of life and functional abilities.
Referências
- Negrini S, Donzelli S, Aulisa AG, et al. "Diretrizes SOSORT 2016: Tratamento ortopédico e de reabilitação da escoliose idiopática durante o crescimento". Escoliose e doenças da coluna vertebral. 2018;13:3. doi: 10.1186/s13013-018-0175-8.
- Hresko MT. "Prática clínica. Escoliose idiopática em adolescentes". N Engl J Med. 2013;368(9):834-841. doi: 10.1056/NEJMcp1209063.
- Trobisch P, Suess O, Schwab F. "Escoliose idiopática". Dtsch Arztebl Int. 2010;107(49):875-883. doi: 10.3238/arztebl.2010.0875.
- Lonstein JE, Carlson JM. "A previsão da progressão da curva na escoliose idiopática não tratada durante o crescimento". J Bone Joint Surg Am. 1984;66(7):1061-1071. doi: 10.2106/00004623-198466070-00008.
- Weiss HR, Moramarco M. “Scoliosis: Treatment indications according to current evidence.” Current Pediatric Reviews. 2013;9(1):37-40. doi: 10.2174/1573396311309010007.
- Weinstein SL, Dolan LA, Cheng JC, et al. "Adolescent idiopathic scoliosis" (Escoliose idiopática do adolescente). Lancet. 2008;371(9623):1527-1537. doi: 10.1016/S0140-6736(08)60658-3.
- Negrini S, Grivas TB, Kotwicki T, et al. “Why do we treat adolescent idiopathic scoliosis? What we want to obtain and to avoid for our patients.” Jornal Europeu da Coluna Vertebral. 2006;15(4):559-570. doi: 10.1007/s00586-005-1061-z.
- Qiu Y, Zhu F, Wang WJ, et al. “Radiological classification and risk factors for curve progression in idiopathic scoliosis.” Jornal Europeu da Coluna Vertebral. 2008;17(9):1327-1339. doi: 10.1007/s00586-008-0702-3.
- Skaggs DL, Guillaume TJ, El-Hawary R, et al. "Nonoperative treatment for idiopathic scoliosis." J Bone Joint Surg Am. 2021;103(13):1221-1231. doi: 10.2106/JBJS.21.00341.
- Watanabe K, Hosogane N, Toyama Y, et al. “Optimal treatment strategy for non-structural scoliosis in children and adolescents.” Jornal Asiático da Coluna Vertebral. 2011;5(2):132-139. doi: 10.4184/asj.2011.5.2.132.