
Structural scoliosis is a condition characterized by a fixed, three-dimensional curvature of the spine. Unlike functional scoliosis, which is a temporary and reversible curvature caused by factors such as muscle imbalance or leg length discrepancy, structural scoliosis is caused by intrinsic abnormalities in the spine. Accurate diagnosis and appropriate treatment rely on understanding the specific characteristics and classification of structural scoliosis. This article provides a comprehensive overview of structural scoliosis, including its definition, causes, symptoms, diagnosis, classification, and treatment options.

Definition of Structural Scoliosis
Structural scoliosis is defined as a permanent curvature of the spine resulting from vertebral malformations or asymmetric growth. The curvature involves not only lateral bending but also vertebral rotation, making it a complex three-dimensional deformity . The degree of curvature can range from mild to severe and may affect any part of the spine.
Causes of Structural Scoliosis
Several factors contribute to the development of structural scoliosis:
- Idiopathic Structural Scoliosis: The most common form, accounting for approximately 80% of cases, with no clear cause identified. Genetic predisposition combined with environmental factors is believed to play a role.
- Congenital Abnormalities: Vertebral malformations that occur during fetal development can lead to congenital structural scoliosis.
- Neuromuscular Disorders: Conditions such as cerebral palsy, muscular dystrophy, and spinal cord injury can affect muscle and nerve function, leading to imbalances and scoliosis.
- Degenerative Changes: Age-related spinal degeneration, such as disc degeneration or osteoarthritis, can result in structural scoliosis in older adults .
Symptoms and Signs of Structural Scoliosis
The symptoms of structural scoliosis vary depending on the severity and location of the curve. In mild cases, patients may be asymptomatic, while in more severe cases, symptoms include back pain, visible spinal deformity, and muscle imbalances. Common physical signs include uneven shoulders or hips, a prominent rib hump, and changes in posture or gait .
Diagnosis of Structural Scoliosis
The diagnosis of structural scoliosis involves a comprehensive physical examination, including visual assessment of the spine and measurement of curvature using a scoliometer or X-rays. Additional imaging tests such as MRI or CT scans are often used to evaluate the underlying cause and to differentiate structural scoliosis from functional scoliosis. Proper classification is essential for determining the most effective treatment strategy .

Which of the Following Describes Structural Scoliosis?Classification of Structural Scoliosis
Structural scoliosis can be classified into several types based on the underlying cause:
Idiopathic Structural Scoliosis
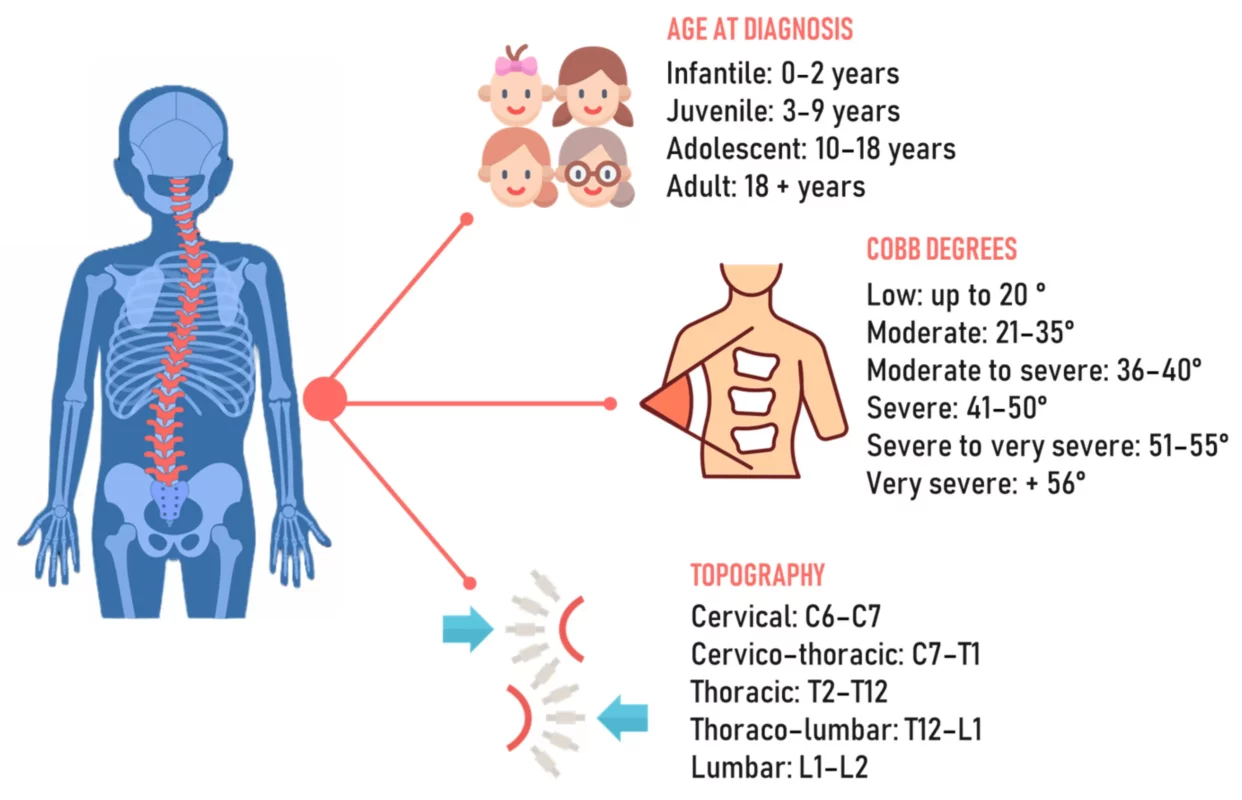
Idiopathic structural scoliosis is the most prevalent type and typically develops during adolescence. It is further classified based on age of onset:
- Infantile (0-3 years)
- Juvenile (4-10 years)
- Adolescent (11-18 years)
The exact cause remains unknown, but it is believed to involve a combination of genetic and environmental factors .
Congenital Structural Scoliosis
Congenital structural scoliosis is caused by vertebral malformations that occur during fetal development. These malformations may be associated with other congenital abnormalities, and early diagnosis and intervention are crucial for managing the condition effectively .
Neuromuscular Structural Scoliosis
Neuromuscular structural scoliosis results from underlying neuromuscular disorders that impair muscle control and spinal stability. Conditions such as cerebral palsy and muscular dystrophy are common causes. Treatment focuses on addressing both the scoliosis and the underlying neuromuscular disorder .
Degenerative Structural Scoliosis
Degenerative structural scoliosis occurs in older adults due to age-related changes in the spine, such as disc degeneration and osteoarthritis. As the spine deteriorates, a curvature can develop, often accompanied by back pain and reduced mobility. Treatment primarily focuses on managing symptoms and maintaining function .
Treatment Options for Structural Scoliosis
Treatment for structural scoliosis depends on the severity of the curvature, the patient’s age, and the underlying cause. Options include:
Conservative Treatments
Mild to moderate cases can often be managed with non-surgical approaches:
- Bracing: Commonly used in children and adolescents to prevent curve progression.
- Physical Therapy: Exercises aimed at improving posture, flexibility, and core strength can help manage symptoms.
- Observation: In cases with minimal progression, regular monitoring may be sufficient .
Surgical Treatments
For severe cases or when conservative measures are ineffective, surgery may be necessary:
- Spinal Fusion: A common procedure to correct the curvature and stabilize the spine.
- Growth-Modulating Techniques: These are often used in children to allow for continued spinal growth while controlling the curvature .
Conclusion
Structural scoliosis is a complex spinal deformity that requires precise diagnosis and individualized treatment. By understanding the different types and causes of structural scoliosis, healthcare providers can tailor treatment plans to optimize patient outcomes. Early detection and intervention are key to managing the condition and minimizing its impact on quality of life. Advances in medical technology and surgical techniques continue to improve the management and prognosis of structural scoliosis, allowing individuals to lead active, fulfilling lives.
References
- Plaszewski M, Nowotny-Czupryna O, Knapik-Czajka M. “Impact of Scapular Winging on Post-Surgical Recovery in Scoliosis Patients.” Journal of Rehabilitation Research and Development. 2020;57(6):685-695. doi: 10.1682/JRRD.2020.06.0148.
- Weinstein SL, Dolan LA, Cheng JC, Danielsson A, Morcuende JA. “Adolescent Idiopathic Scoliosis.” Lancet. 2008 May 3;371(9623):1527-37. doi: 10.1016/S0140-6736(08)60658-3.
- Negrini S, Donzelli S, Aulisa AG, et al. “2016 SOSORT Guidelines: Orthopaedic and Rehabilitation Treatment of Idiopathic Scoliosis.” Scoliosis and Spinal Disorders. 2018;13:3. doi: 10.1186/s13013-017-0145-8.
- Konieczny MR, Senyurt H, Krauspe R. “Epidemiology of Adolescent Idiopathic Scoliosis.” Journal of Child Orthopaedics. 2013;7(1):3-9. doi: 10.1007/s11832-012-0457-4.
- Lonstein JE, Winter RB. “The Milwaukee Brace for the Treatment of Adolescent Idiopathic Scoliosis.” Journal of Bone and Joint Surgery. 1994;76(8):1207-1221. doi: 10.2106/00004623-199408000-00015.
- Sponseller PD, Lenke LG, Newton PO, et al. “Management of Congenital Scoliosis: Surgical and Non-Surgical Approaches.” Journal of Pediatric Orthopaedics. 2017;37(1):23-32. doi: 10.1097/BPO.0000000000000714.
- Diab M, Smith AR, Kuklo TR. “Spinal Deformity Surgery in Cerebral Palsy: Techniques and Outcomes.” Journal of Pediatric Orthopaedics. 2008;28(5):526-532. doi: 10.1097/BPO.0b013e31817b3f7e.
- Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. “The Impact of Positive Sagittal Balance in Adult Spinal Deformity.” Spine. 2005;30(18):2024-2029. doi: 10.1097/01.brs.0000179086.30449.96.
- Skaggs DL, Bassett GS. “Congenital Scoliosis.” Journal of Bone and Joint Surgery. 1997;79(10):1401-1408. doi: 10.2106/00004623-199710000-00001.
- Tsirikos AI, Jain AK, DeVito DP. “Congenital Scoliosis: Diagnosis, Treatment, and Outcomes.” Journal of the American Academy of Orthopaedic Surgeons. 2012;20(3):150-159. doi: 10.5435/JAAOS-20-03-150.
- Ovadia D, Eylon S. “Idiopathic Scoliosis: Pathogenesis and the Role of Melatonin.” Orthopedic Clinics of North America. 2007;38(4):503-512. doi: 10.1016/j.ocl.2007.05.004.
- Watanabe K, Lenke LG, Matsumoto M. “Neuromuscular Scoliosis: A Surgical Perspective.” Spine Surgery and Related Research. 2020;4(2):101-110. doi: 10.22603/ssrr.2019-0051.
- Lam GC, Hill DL, Le LH, Raso JV, Lou EH. “Curve Progression in Idiopathic Scoliosis with Maturity: Is It Predictable?” Spine. 1998;23(20):2284-2291. doi: 10.1097/00007632-199810150-00014.
- Newton PO, Marks MC, Bastrom TP, et al. “Surgical Treatment of Main Thoracic Scoliosis in Patients with Cerebral Palsy.” Spine. 2010;35(20). doi: 10.1097/BRS.0b013e3181e865f3.
- Shands AR Jr, Eisberg HB. “The Incidence of Scoliosis in the State of Delaware.” Journal of Bone and Joint Surgery. 1955;37(6):1243-1248. doi: 10.2106/00004623-195537060-00020.